Cardiovascular
Population Intervention Effects of Spatial Social Polarization on Hypertension Disparities Hoda Abdel Magid* Hoda Abdel Magid Mengya Xu Gina S. Lovasi Suzanne Judd Michelle C. Odden
Background: Spatial social polarization (SSP)—the unequal geographic distribution of privilege and deprivation—is hypothesized to drive hypertension disparities in the United States. Using the Index of Concentration at the Extremes (ICE), SSP was measured across six domains: income, education, homeownership, primary language, race/ethnicity, and joint race/ethnicity with income. This study used 2019 claims data (N=644,707) to estimate the population-level impact of eliminating SSP disparities on hypertension outcomes through counterfactual modeling in Black and White adults.
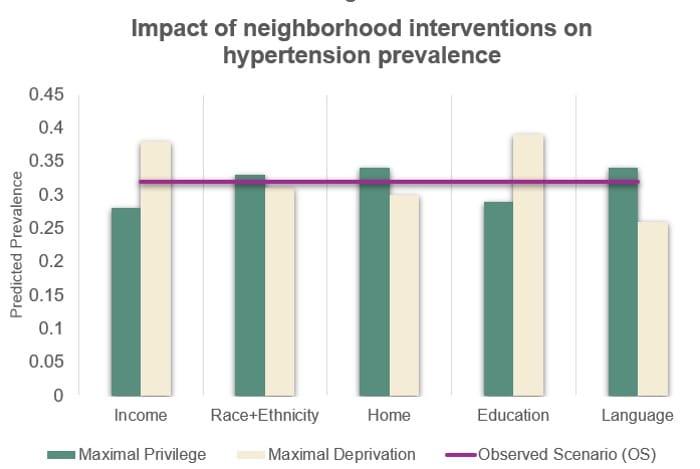
Methods and Results: Population Intervention Models (PIMs) with the parametric g-formula simulated counterfactual scenarios where SSP disparities were eliminated, allowing comparisons of current exposure levels with idealized distributions (e.g., universal privilege or deprivation). Analyses at the ZIP code level were adjusted for demographic factors and clinical comorbidities, including diabetes, hyperlipidemia, and myocardial infarction. Observed hypertension prevalence was 32%. Results demonstrated significant SSP-related gradients. In a hypothetical scenario where everyone lived in high-income neighborhoods, hypertension prevalence would decrease by 4.3%, while residence in income-deprived areas would increase prevalence by 5.8%. Neighborhood racial composition effects varied: among White participants (70% of the sample), moving to predominantly White neighborhoods increased prevalence from 33.2% to 33.6%. Among Black participants (11%), relocating to predominantly White neighborhoods decreased prevalence by 0.3%, while residence in predominantly Black neighborhoods increased prevalence by 0.3%. Living in neighborhoods with higher educational attainment reduced hypertension prevalence by 3.8%, while residence in neighborhoods with lower educational attainment increased it by 6.3%.
Conclusion: Eliminating SSP disparities could significantly reduce hypertension prevalence, with the greatest benefits observed in socioeconomically deprived communities. These findings highlight SSP as a critical determinant of hypertension disparities and underscore the potential for targeted, neighborhood-level interventions to reduce polarization and advance cardiovascular health equity