Injuries/Violence
Assessing the concurrent validity of firearm-related mortality estimates from the Global Burden of Disease studies Sid Zadey* Sid Zadey Christopher N. Morrison
Background: Global Burden of Disease (GBD) studies are dominant in global public health and policymaking as they comprehensively model epidemiological parameters for 380+ conditions and injuries in 200+ countries over 30 years. GBD models have been criticized for being challenging to interpret, agnostic to theoretical nuances with limited work on the concurrent validity. We aimed to fill this gap using the firearm mortality outcomes for the United States (US), which are known to have accurate reporting at the state-level by the US Centers for Disease Control and Prevention (CDC).
Methods: We used US CDC WONDER and the GBD 2019 study as the sources for observed and estimated data. Data were extracted for mortality rates per 100000 people for all ages and both sexes for 50 US states and the District of Columbia from 2000-2019 for suicides, homicides, and unintentional injuries involving firearms. Outcome-wise validation was conducted using the Lin’s concordance correlation coefficient (CCC). CCC >0.99 is considered ‘almost perfect’ agreement, 0.95-0.99 is considered substantial, 0.90-0.95 is moderate and <0.90 is poor. Analysis and visualization were conducted in R.
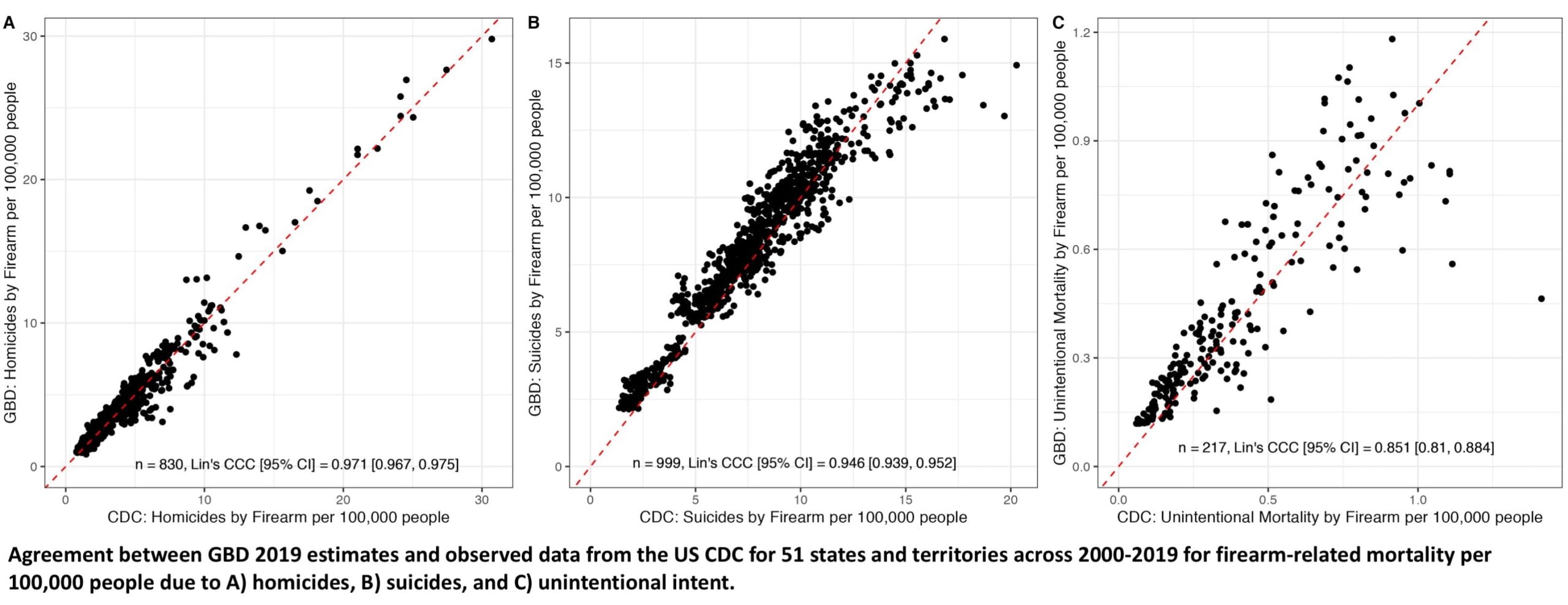
Results: Available data points across the three outcomes varied since the underlying count data for firearm-related mortality were suppressed or unreliable for certain states and years. Hence, our analytical dataset contained 2046 data points (67% of the total data). Lin’s CCC revealed that agreements between the GBD estimates and CDC observations were substantial, moderate, and poor for homicide (n=830, CCC [95%CI]=0.971 [0.967, 0.975]), suicide (n=999, CCC=0.946 [0.939, 0.952]), and unintentional (n=217, CCC=0.851 [0.81, 0.884]) firearm-related mortality rates (Figure 1A-C). For firearm-related suicide mortality rates, the deviation between sources was larger for higher values noting underestimation by GBD (Figure 1B).
Conclusion: We chose firearm violence measures for validation due to their reliable reporting in a high-income country with relatively high mortality and public significance. For this, we found that concurrent validity of estimates from the GBD study may vary across outcomes, geographies and periods.
Significance: To our knowledge, this is the first such validation effort for any injury outcome from the GBD study. This cursory assessment should encourage more rigorous validation efforts to understand the appropriate use of and post hoc corrections to GBD estimates.