Population-level indirect protection from COVID-19 vaccine-derived immunity across spatial scales
Abstract
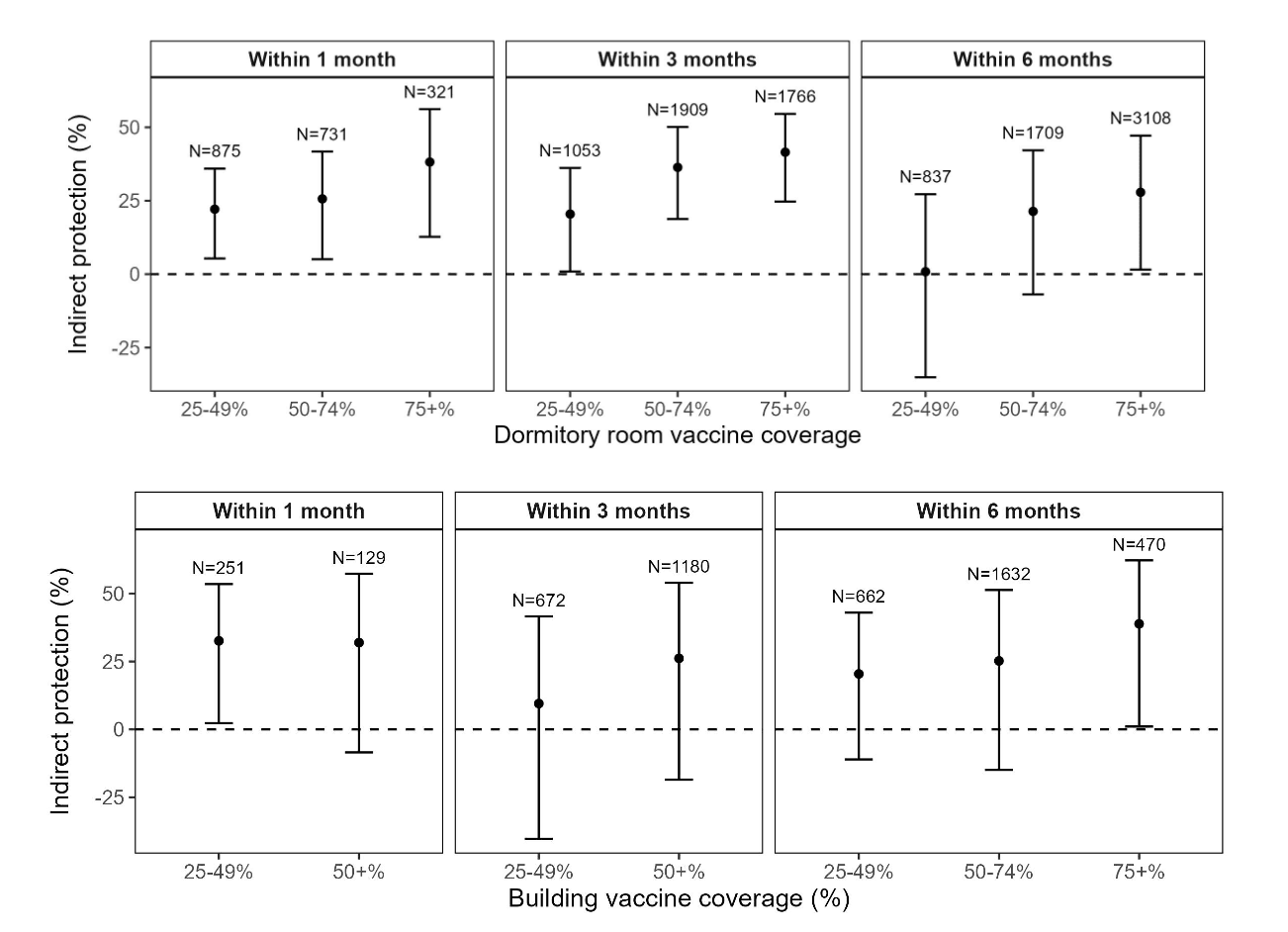
Despite years of COVID-19 vaccination, the extent to which COVID-19 vaccines confer indirect protection at the population level remains poorly characterized. Indirect protection, defined as reduced infection risk among close contacts of vaccinated individuals, is key to understanding population transmission and informing vaccine policy. While observational studies at small spatial scales (e.g., households, shared prison cells) have demonstrated moderate indirect protection from COVID-19 vaccines, there remains limited understanding of how vaccine-derived indirect protection shapes transmission at broader spatial scales. Here, we show that higher and more recent COVID-19 vaccination coverage was associated with progressively greater indirect protection against SARS-CoV-2 infection. Analyzing longitudinal de-identified surveillance data (December 2020–December 2022) from 35 California state prisons, we estimate indirect vaccine protection at two spatial scales defined as dormitory rooms (mean: 25 persons, IQR: 6-22) and large buildings (mean: 153 persons, IQR: 109-169). Compared to dormitory rooms with <25% vaccine coverage within the past 3 months, indirect protection was estimated to be 21% (95% CI: 1–36%) in dormitory rooms with 25–49% coverage, 36% (19–50%) with 50–74% coverage, and 42% (25–55%) with ≥75% coverage. Indirect protection was attenuated when using a 6-month vaccination window [28% (2–47%) with ≥75% coverage]. At the building level, we observed more variable protection, with 39% (1–62%) indirect protection at ≥75% vaccine coverage within 6 months. These findings provide evidence of population-level indirect protection from COVID-19 vaccination, estimating stronger indirect protection in settings facilitating closer social contacts (e.g., dormitory rooms) and potentially more variable protection at larger spatial scales with more diffuse and heterogeneous social mixing (e.g., building), with implications to public health policy and epidemic modeling.