Neighborhood Socioeconomic deprivation and Opioid Prescribing Trends Among Medicare Part D Clinicians: A Five-Year Longitudinal Analysis (2019–2023)
Abstract
Background: Geographic and socioeconomic disparities often drive variations in healthcare delivery. However, it remains unclear if neighborhood-level deprivation independently influences high-risk opioid prescribing among clinicians in pain-related specialties.
Objectives: To determine if the Area Deprivation Index (ADI) is associated with opioid prescribing rates and long-acting (LA) opioid use, and to evaluate if prescribing declines from 2019 to 2023 were uniform across socioeconomic gradients. To assess whether high opioid prescribing clusters with other high‑risk drug classes across the ADI gradient.
Methods: A repeated cross-sectional analysis was conducted using 2019–2023 Medicare Part D prescriber data for clinicians (N=140,519) in pain-related specialties (orthopedics, pain medicine, physical medicine and rehabilitation, and primary care). Residential or practice addresses were geocoded using the U.S. Census Geocoder, with records successfully matched at the census block-group level linked to the Area Deprivation Index (ADI) via 11‑digit block-group FIPS codes; addresses without valid block-group assignments or with ambiguous geocodes were excluded. Outcomes included overall opioid prescribing rates and the proportion of beneficiaries receiving long‑acting opioid formulations. Models adjusted for beneficiary age, sex, race, disability, dual‑eligibility, risk score, and urbanicity. High opioid prescribers were defined as those in the top quartile of opioid volume for a given year, and were compared with respect to high prescribing of antibiotics and antipsychotics.
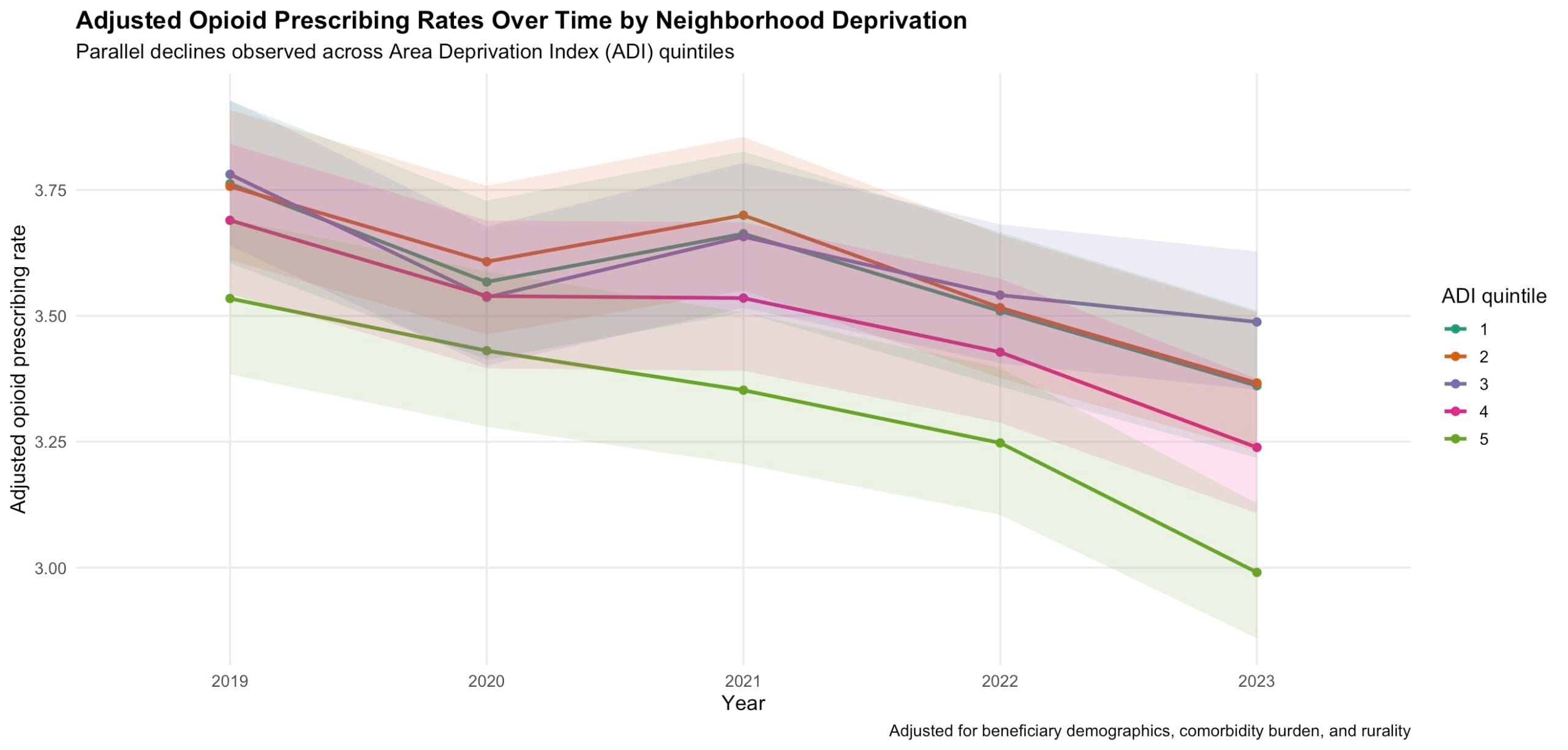
Results: Adjusted opioid prescribing rates declined steadily from 2019 to 2023; compared with 2019, rates were 4.1% lower in 2020, 4.6% lower in 2021, 10.8% lower in 2022, and 14.5% lower in 2023, with no statistically significant difference in the magnitude of decline across ADI quintiles (p for interaction = 0.09).
Across all years, higher neighborhood deprivation was associated with slightly lower opioid prescribing. A 10‑point increase in ADI was associated with a 1.24% decrease in opioid prescribing rate (95% CI, 1.86%–0.62% decrease; p<0.001). The adjusted proportion of beneficiaries receiving long‑acting opioids declined from 7.28% at the 10th percentile of ADI to 5.56% at the 90th percentile (1.72 percentage‑point absolute and ~24% relative reduction; p<0.001 across the ADI gradient).
Within individual specialties, ADI associations were attenuated and not statistically significant, consistent with reduced power and control for between‑specialty practice differences.
High opioid prescribers were more likely to also be high prescribers of antibiotics (27.6% vs 20.3%) and antipsychotics (21.9% vs 9.9%), with clustering most pronounced in deprived neighborhoods; in the highest ADI quintile, the adjusted probability of high antipsychotic prescribing among high opioid prescribers was 34.8% versus 12.5% among other prescribers (p for interaction<0.001).
Conclusions: Among Medicare Part D clinicians in pain-related specialties higher neighborhood deprivation was associated with lower rates of long-acting opioid prescribing, suggesting under‑treatment or access barriers in deprived areas rather than excess high‑risk opioid prescribing, while concentrated multi‑drug high‑risk prescribing in these neighborhoods highlights priority targets for intervention.