Prevalences of United States Preventive Services Task Force-recommended cancer screenings in older adults with Medicare Advantage versus traditional Medicare
Abstract
Background: Medicare Fee for Service (FFS) claims are an established resource for epidemiologic research while the utility of Medicare Advantage (MA) data, only made available for research in 2019, remains largely unexamined. To address this, we compared standardized prevalences of cancer screenings in MA encounter vs FFS claims data.
Methods: We used Medicare enrollment, claims, and encounter data linked with the National Health and Aging Trends Study (NHATS), a nationally-representative cohort of Medicare beneficiaries >65 years. Round 7 (2017) NHATS interview participants with continuous enrollment in Medicare for 365 days (‘pre-index period’) before the interview were included. We identified cancer screenings using ICD-10 diagnosis codes and defined participants with >1 code during the pre-index period as ‘screened’. To account for differences in the beneficiary populations, we standardized FFS beneficiaries to MA beneficiaries by age, gender, race, ethnicity, rurality, education, frailty, dementia, comorbidities, smoking, sensory impairment, falls, and hospitalizations measured in NHATS. We estimated the prevalence difference (PD) and 95% confidence interval (CI) for colorectal cancer screening, breast cancer screening (among women), and prostate cancer screening (among men) in MA vs FFS data.
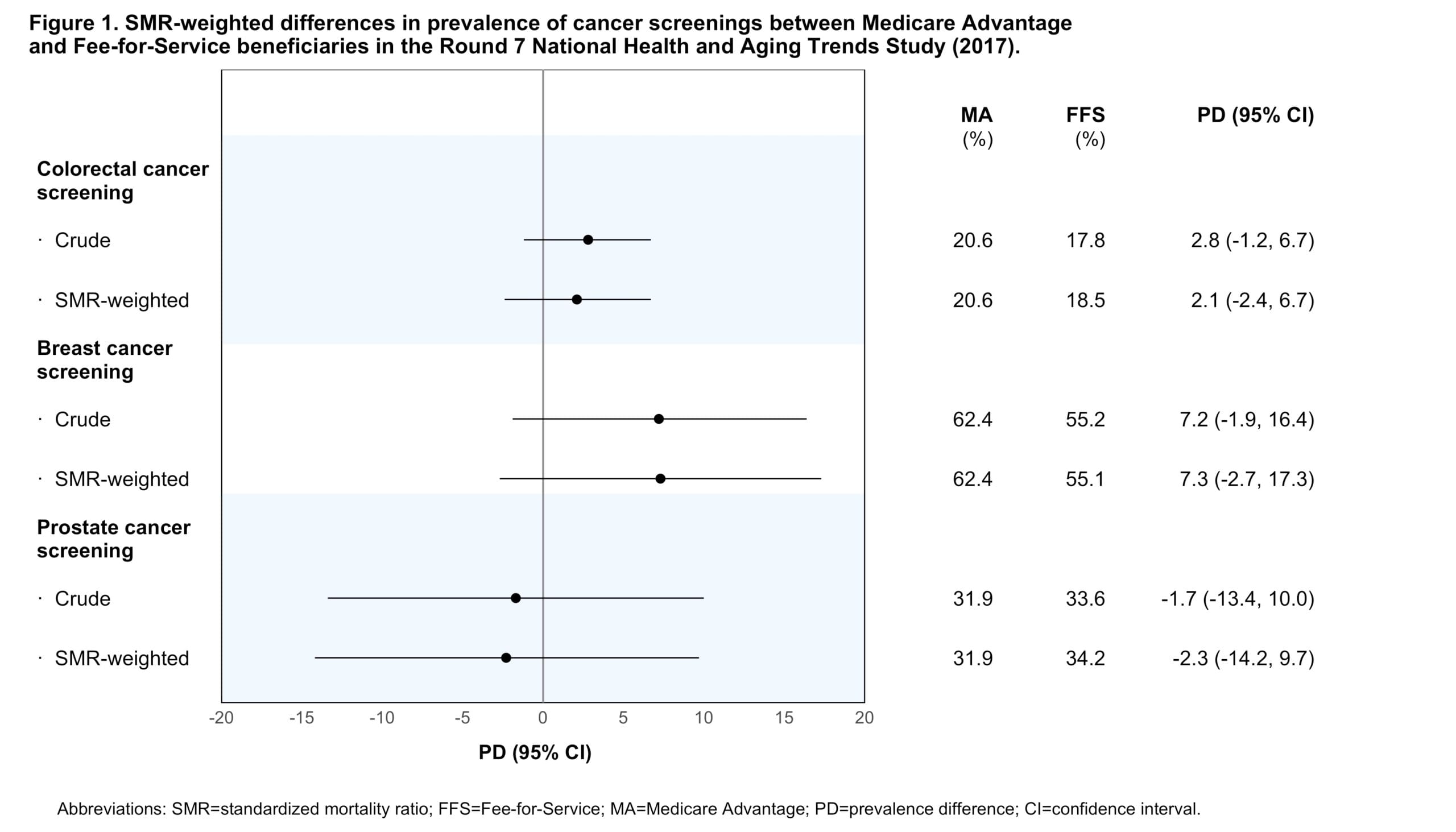
Results: Of the 4,804 beneficiaries in our cohort (median age 74 years, 56% female), 40% had MA and 60% had FFS plans. MA beneficiaries were more likely to be Black, Hispanic, have less than a high school degree, and reside in a metropolitan area. Comparing MA to FFS data, standardized prevalence differences were 2.1% (95% CI -2.4–6.7%) for colorectal cancer screening, 7.3% (95% CI -2.7–17.3%) for breast cancer screening, and -2.3% (95% CI -14.2–9.7%) for prostate cancer screening. Crude estimates were similar.
Conclusions: Cancer screening prevalences were comparable between MA and FFS, supporting the use of MA encounter data for epidemiologic research among older adults.