Characterization of sexual partnerships and prediction of future age distribution and HIV burden in Botswana and Zambia: preliminary findings from the EPIPLAN-HIV model
Abstract
Introduction: HIV prevalence has shifted to older ages due to longer lifespans among people with HIV and lower incidence in younger ages. Past modeling has underestimated this age shift and has underassessed sexual partnerships in older adults. Using repeated population-based surveys in Botswana and Zambia, we describe sexual partnerships and model HIV prevalence by 2040.
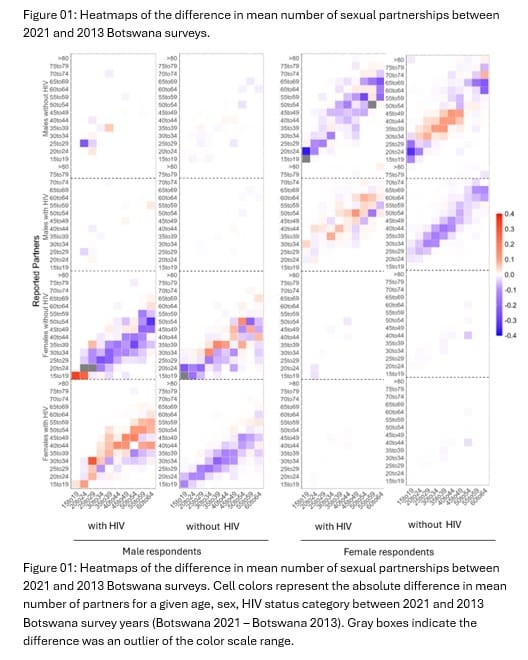
Methods: Using Population-based HIV Impact Assessment (PHIA) survey data from Botswana (2013, 2021) and Zambia (2016, 2021), participants age ≥15 years (y) reported sexual partnerships in the past year and underwent HIV testing. We report weighted mean and 95% CIs for sexual partners by sex, age, and HIV status (Fig 01). Extending an age-based cohort model to include HIV acquisition risk stratified by age and sex based on partner profiles, we projected HIV prevalence by age for each country independently.
Results: In Botswana 2021, people with (vs. without) HIV had fewer partnerships [men: 0.97 (95% CI: 0.89, 1.04) vs 1.27 (1.22, 1.31); women: 0.85 (0.81, 0.89) vs 0.96 (0.92, 0.99)]. In Zambia 2016, men with (vs. without) HIV had more partnerships [1.13 (1.06, 1.21) vs 1.00 (0.97, 1.03)]. From 2013 to 2021 in Botswana, serodifferent partnerships decreased and seroconcordant partnerships increased (Fig 01). In Zambia 2021, adults ≥50y had higher prevalence of serodifferent partnerships versus adults <50y [10.85% (7.86%, 13.84%) vs 6.29% (5.34%, 7.24%)]. Trends were similar but with overlapping confidence intervals in Botswana 2021. By 2040, we predict the HIV prevalence in Botswana and Zambia will be 6% and 2%, respectively and HIV prevalence among adults ≥50y will be 32% and 30%, respectively.
Conclusions: Older age was associated with serodifferent partnerships in Zambia. We predict by 2040, ≥30% of adults ≥50y in each country will have HIV. HIV testing and prevention programs may need to include programming for older adults to achieve and maintain epidemic control.