Associations between initial treatments for low-back pain and opioid use disorder risk in Medicaid patients
Abstract
Introduction: Acute low back pain is a leading cause of disability worldwide, and despite guidelines cautioning against it, opioid prescribing remains common for this condition. Initial treatment modalities for low back pain range from pharmacologic to non‑pharmacologic therapies, each carrying different levels of risk for later developing opioid use disorder (OUD). We studied the incidence of OUD in an opioid‑naïve, Medicaid‑insured adult population with newly diagnosed acute low back pain and estimated the association between initial treatment modalities and subsequent OUD risk.
Methods: Using Medicaid T‑MSIS analytic files from 25 states (2016–2019), we identified opioid‑naïve adults with a new diagnosis of acute low back pain who received any pharmacologic or non‑pharmacologic treatment within one month. Associations between initial treatment modality and OUD risk were estimated using a non‑parametric, doubly robust estimator.
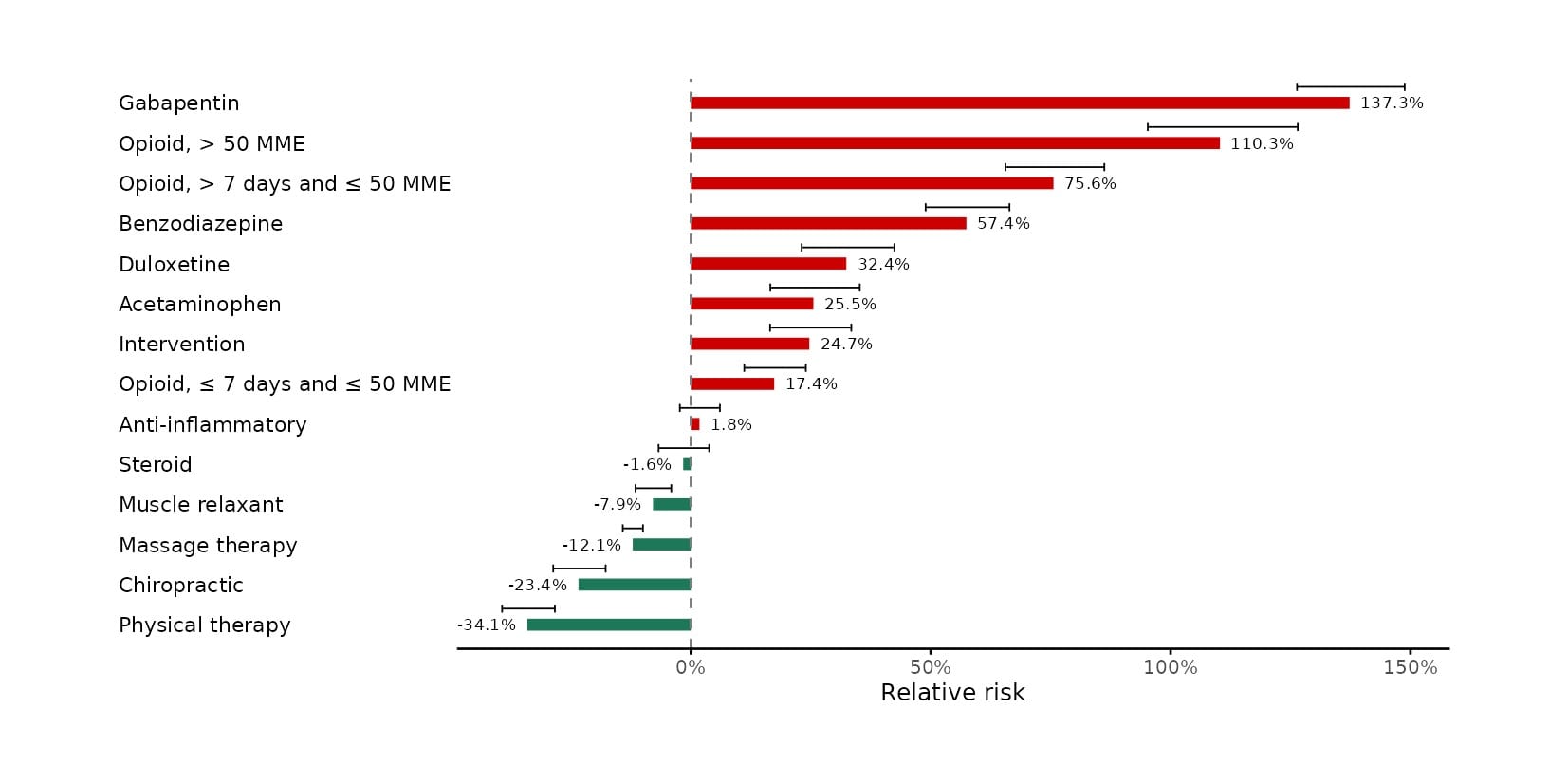
Results: The cohort consisted of 574,196 opioid‑naïve adults initiating treatment for low back pain. OUD incidence at the end of 9 and 15 months of follow‑up was 1.8% and 3.51%, respectively. Gabapentinoids were associated with the highest increase in OUD risk (137.3%, 95% CI: 126.4%, 148.8%), followed by higher‑dose opioids, defined as >50 Morphine Milligram Equivalents (MME) (110.3%, 95% CI: 95.2%, 126.5%). Lower‑dose short‑duration opioids (≤50 MME, ≤7 days) were also associated with elevated risk, though substantially smaller in magnitude (7.4%, 95% CI: 11.1%, 24.0%). All non‑pharmacologic therapies were associated with reduced OUD risk, with physical therapy being associated with the largest risk reduction of 34.1% (95% CI: –39.3%, –28.3%).
Discussion: In opioid‑naïve Medicaid patients experiencing low back pain, non‑pharmacologic treatment modalities were associated with reduced OUD risk. Gabapentinoids and opioid use were each associated with increased risk; for opioids, the degree of risk increased with higher doses and durations.