The association between sickle cell trait, a prevalent genetic condition, and the risk of preterm birth in a pregnancy cohort
Abstract
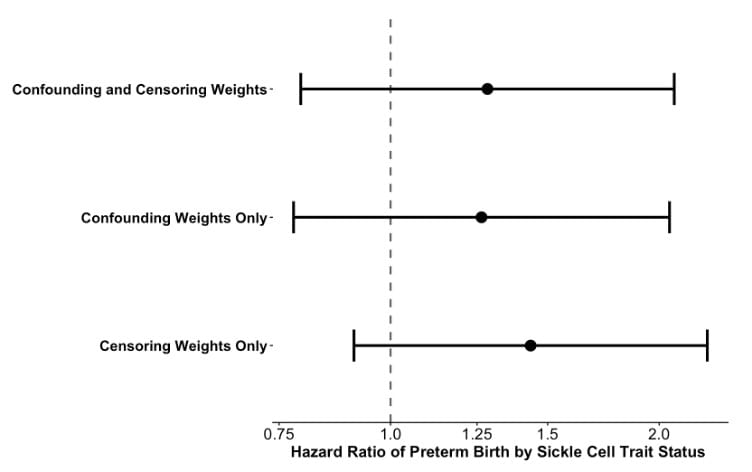
Associations between preterm birth and sickle cell trait (SCT) have been reported, yet few studies account for selection into SCT prenatal screening and competing risk of fetal loss. SCT is prevalent among individuals with African ancestry (7–10%), making rigorous evaluation of its role in preterm birth important for population attributable risk. We evaluated the association between SCT and preterm birth in a pregnancy cohort derived from electronic health records of over 32,000 pregnancies in Black/African American women receiving care at the University of North Carolina Healthcare system. Analyses included 2,080 pregnancies with laboratory-confirmed SCT status (positive or negative) from 2014–2024. Gestational age and pregnancy outcome algorithms were used to construct discrete pregnancy episodes followed over time. Pregnancies with conception dates occurring >19 weeks before data collection began or >43 weeks before data collection ended were excluded. Preterm birth was defined as delivery at ≥22 and <37 completed weeks’ gestation. Cox proportional hazards models with inverse probability of censor weights accounted for censoring and the competing risk of fetal loss. Risks were estimated using the Aalen–Johansen estimator. Inverse probability of treatment weights adjusted for SES, maternal age, prenatal care, BMI, and prenatal screening recommendation at year of conception. In analyses accounting for censoring or competing risks due to fetal loss, but not selection into SCT prenatal screening and confounding, SCT had a modest association with higher risk of preterm birth (hazard ratio [HR] = 1.45; 95% CI: 0.90, 2.27), which was attenuated after applying inverse probability of treatment weights to control for (HR = 1.26; 95% CI: 0.78, 2.05). These findings highlight the importance of accounting for selection into prenatal screening and confounding when evaluating genetic risk factors for adverse pregnancy outcomes in pregnancy cohorts.