Patient-Reported Equity Experiences, Care Setting, and Timely Mammography in an Urban Hospital in Central Brooklyn
Abstract
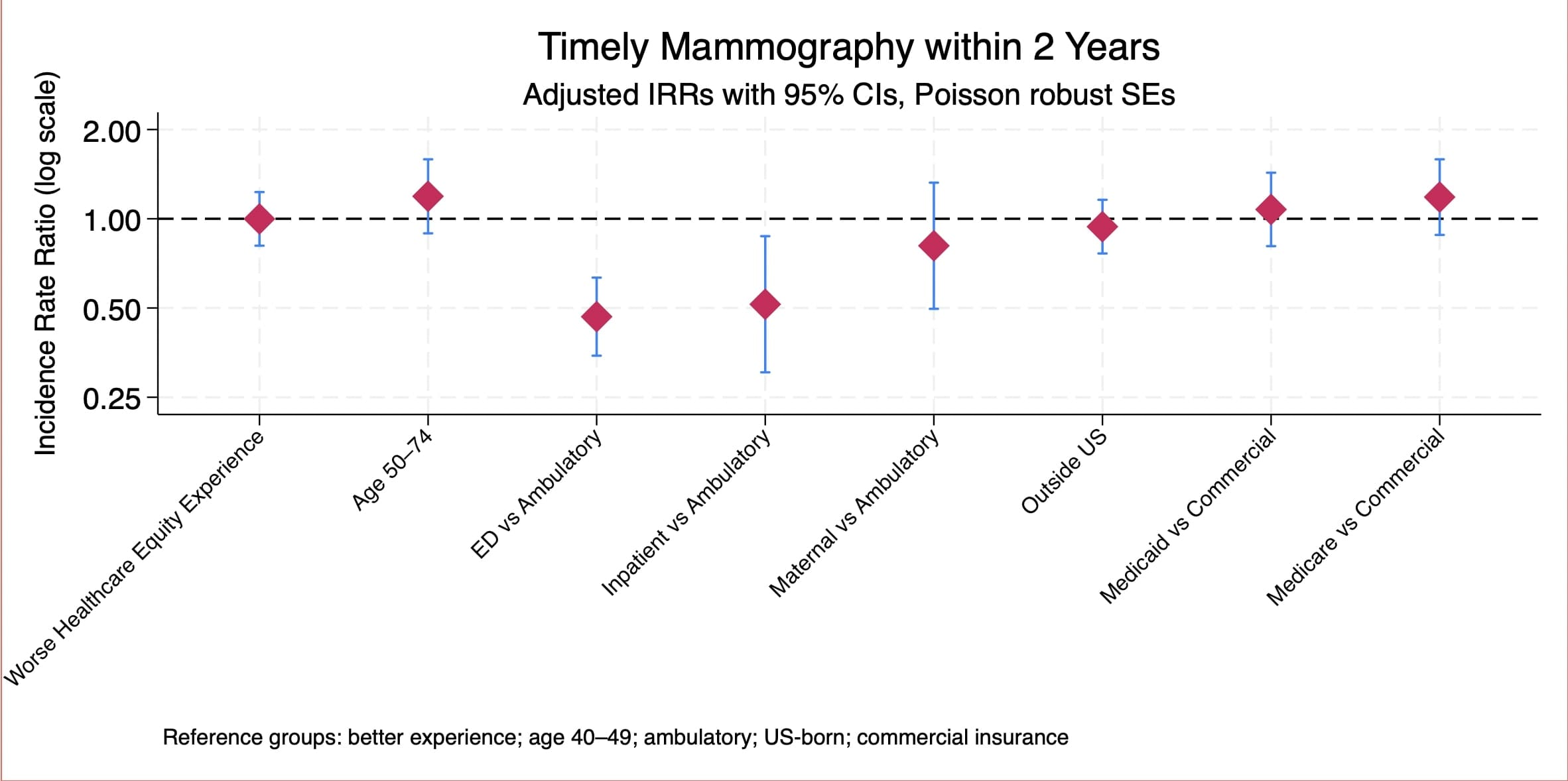
Despite improvements in guideline-based care, disparities in breast cancer screening rates persist. The objective of this study was to determine whether negative healthcare equity experiences are associated with delays in breast cancer screening rates in an urban hospital system. We conducted a longitudinal observational analysis linking health equity experience data from the Brooklyn Health Equity Index (BKHI) survey to EHR records of mammography completion over a two-year follow-up period. The final sample included 678 women aged 40–74, who completed the 10-item BKHI during an index hospital encounter at a central Brooklyn health system and were eligible for breast cancer screening. Patient health equity experience was summarized using latent class analysis (LCA) to identify 2 common experience profiles. The outcome was timely mammography, defined as receipt of screening within two years of the index encounter. We used multivariable Poisson regression with robust standard errors, and adjusted for age, care-setting, nativity, and insurance coverage type. Participants were predominantly Black (91.0%), aged 50–74 years (78.5%), and publicly insured (Medicaid 42.6%; Medicare 32.0%), and 34.2% completed a mammogram. Latent patient experience class was not associated with timely mammography after adjustment (IRR 1.00; 95% CI 0.81–1.23). However, care setting showed strong associations, with emergency department encounters (IRR 0.47; 95% CI 0.35–0.63) and inpatient encounters (IRR 0.51; 95% CI 0.30–0.87) associated with lower screening rates, compared to ambulatory encounters. Age group, nativity, and insurance type were not independently associated with screening in adjusted models. Our models showed no statistically significant difference by health equity experience class, and improvements in breast cancer screening rates may need to focus on care-setting specific processes that support preventive follow-up, in addition to patient health equity experience.