Using a standardized interpretation tool and statistical clustering to inform cardiopulmonary exercise testing interpretation and application
Abstract
Background: Resting pulmonary function tests underestimate functional impairment in deployed veterans with exertional dyspnea. Cardiopulmonary exercise testing (CPET) is more sensitive for characterizing exercise abnormalities, but interpretation is challenging. We developed a standardized CPET scoring tool to classify primary causes of exercise limitation and compared statistical clustering as an alternative approach that may minimize discordant interpretations.
Methods: Two expert pulmonologists independently scored 280 CPETs from dyspneic veterans as normal or primarily a cardiac, ventilatory, gas exchange or metabolic limitation to exercise, with a third pulmonologist adjudicating disagreements. We standardized 24 rest and exercise variables using inverse hyperbolic sine (Asinh), removed tests with incomplete data (n=36), and applied K-means clustering in R with n=1 to 100 clusters.
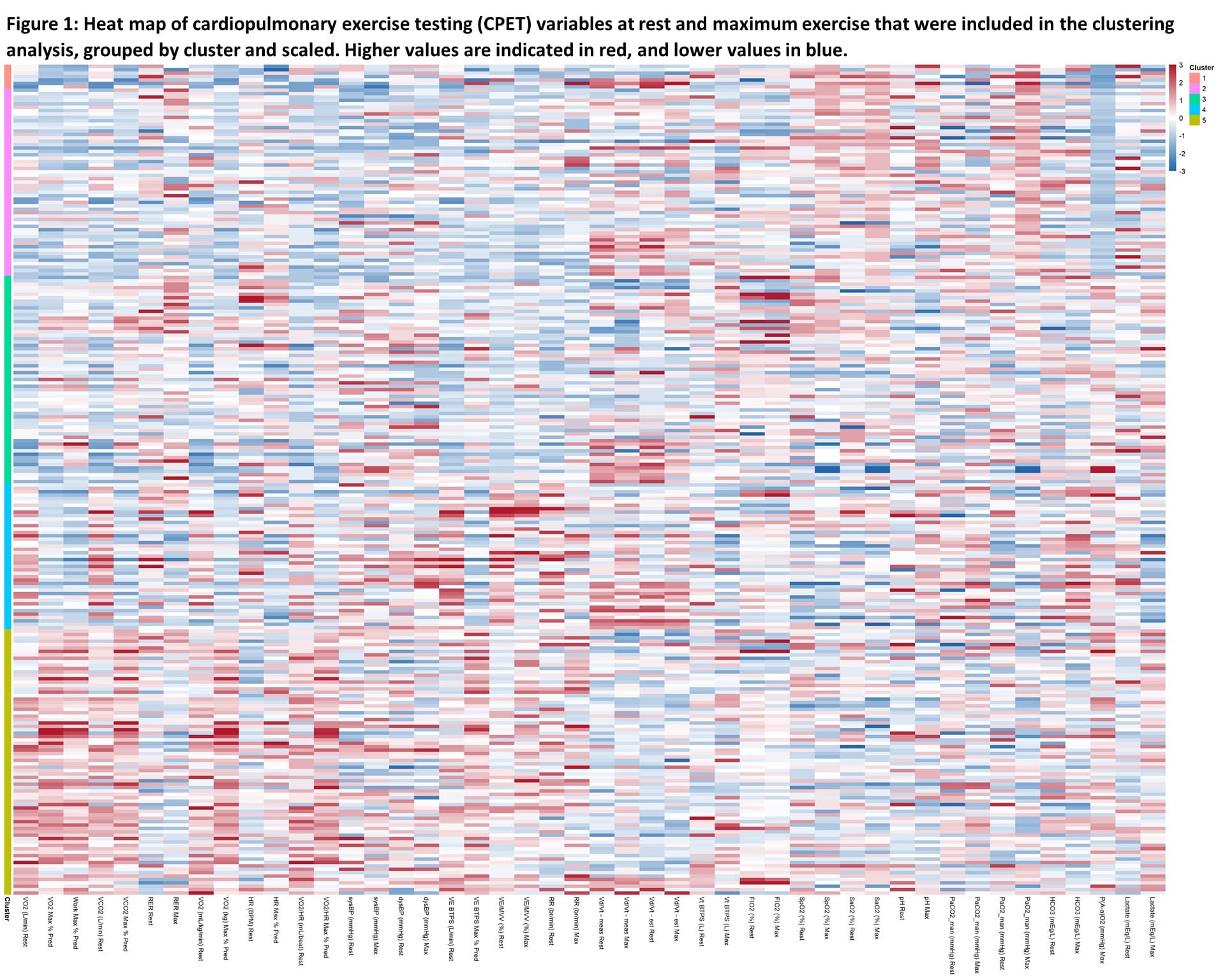
Results: The primary exercise limitation by initial expert scoring was discordant in 151/280 (54%). Tiebreak scoring will be compared to the statistical classification method upon completion. Within-cluster variation was minimized near n=5 clusters. Figure 1 shows included variables by cluster. Cluster 1 (n=7) reflects sub-maximal tests. Clusters 2 (n=55) and 3 (n=61) are similar, with reduced maximum oxygen consumption (VO2max), but 2 appears metabolic (deconditioning or mitochondrial dysfunction) while 3 appears cardiac with reduced oxygen pulse (VO2/HR). Cluster 4 (n=43) appears ventilatory-limited with rapid breathing, higher physiologic dead space/tidal volume (Vd/Vt) and maximum ventilation/voluntary ventilation (VE/MVV) at rest, and higher carbon dioxide (PaCO2) at maximum. Cluster 5 (n=78) reflects more normal exercise.
Discussion: A systematic approach is needed to reliably interpret CPET-identified exercise limitations. Efforts to validate this standardized CPET classification system appear promising for enhanced disease phenotyping and management.