Early post-screening diabetes care and 10-year risk of hemodialysis initiation: a target trial emulation
Abstract
Background: Early engagement in diabetes care after screening could prevent kidney failure, but evidence on hard renal endpoints such as hemodialysis is limited.
Methods: We emulated a target trial using the nationwide JMDC Claims Database (>12 million beneficiaries) in Japan (2005–2021). Adults aged 40–74 years with newly screen-detected diabetes (HbA1c ≥6.5% or fasting glucose ≥126 mg/dL) and no history of renal failure or dialysis were eligible. Participants were assigned to: (1) initiating ≥1 diabetes-related visit <1 year after detection (Strategy 1), or (2) no diabetes-related visit <1 year (Strategy 2). To address immortal time bias and selection bias due to censoring, we used a clone–censor–weight approach. Stabilized inverse-probability weights were estimated using >30 baseline confounders (demographics, lifestyle, metabolic parameters including eGFR and proteinuria, and health-seeking behaviors) and time-varying confounders (cumulative healthcare visits, medications). Follow-up started at diabetes detection. Outcome was maintenance hemodialysis initiation. Weighted pooled logistic regression estimated 10-year risk differences (RD) and risk ratios (RR).
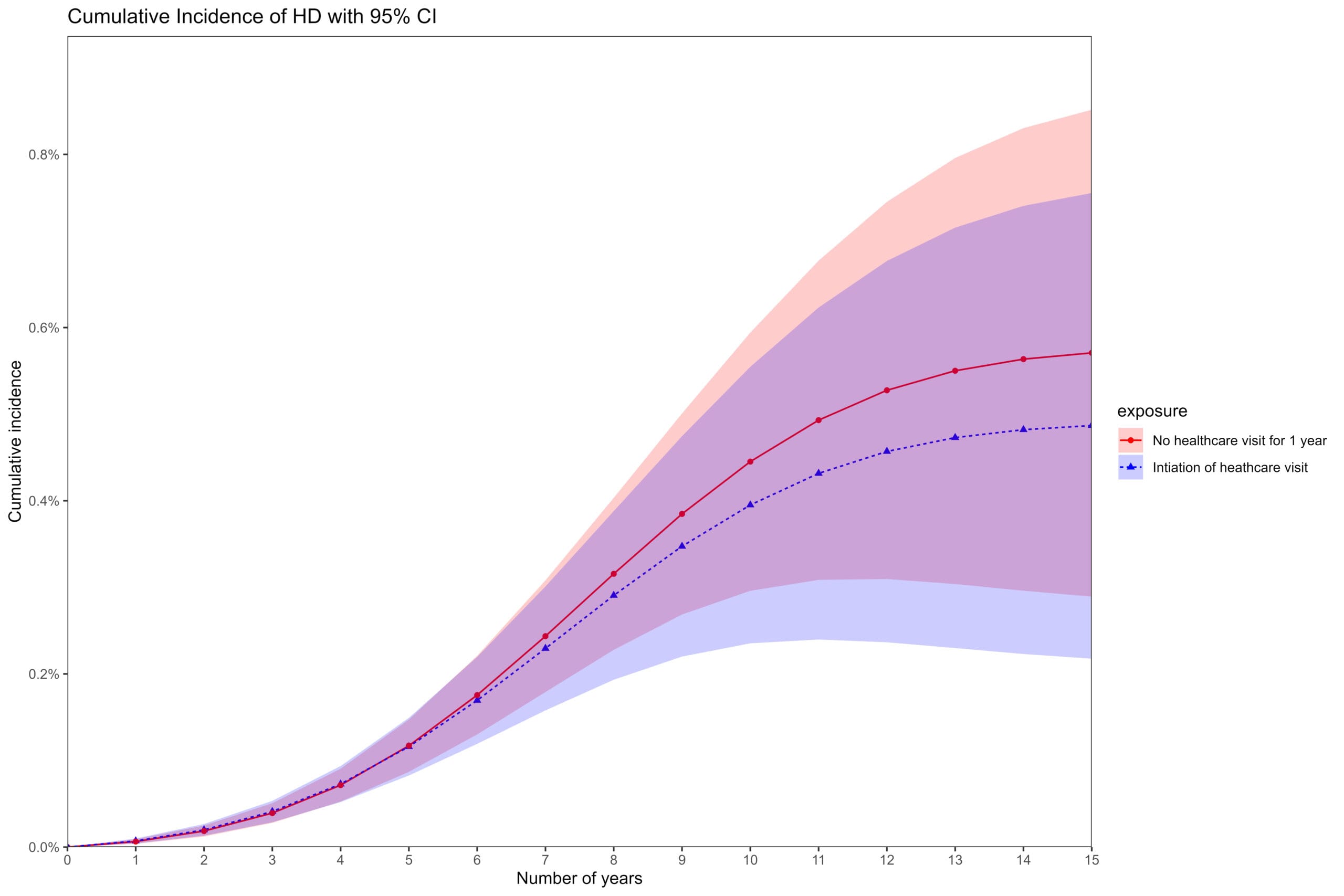
Results: Among 153,455 participants (mean age 53 years; 78% men), 54,278 initiated care <1 year and 71,659 did not; the remainder were censored. Hemodialysis occurred in 74 (Strategy 1) and 54 (Strategy 2) participants (total=128). Early care was associated with RD −0.12 percentage points (95% CI −0.74 to 0.32) and RR 0.94 (95% CI 0.51 to 1.51) at 10 years. Risk curves showed slight separation after approximately 7 years, but confidence intervals substantially overlapped throughout the follow-up.
Conclusions: Among adults with screen-detected diabetes, initiating care <1 year showed no clear association with 10-year hemodialysis risk. Given renal failure’s latency and slight later divergence, longer follow-up is warranted to clarify early engagement’s impact on hard renal outcomes.