Attending Historically Black Colleges or Universities and all-mortality in US Black adults
Abstract
INTRODUCTION
Higher education strongly predicts reduced risk of mortality yet evidence suggests heterogeneity in health returns to education. Black adults may derive long-term health benefits from attendance at an Historically Black College or University (HBCU) compared to attending a Predominantly White Institution (PWI). No prior study has evaluated all-cause mortality in a nationwide sample.
METHODS
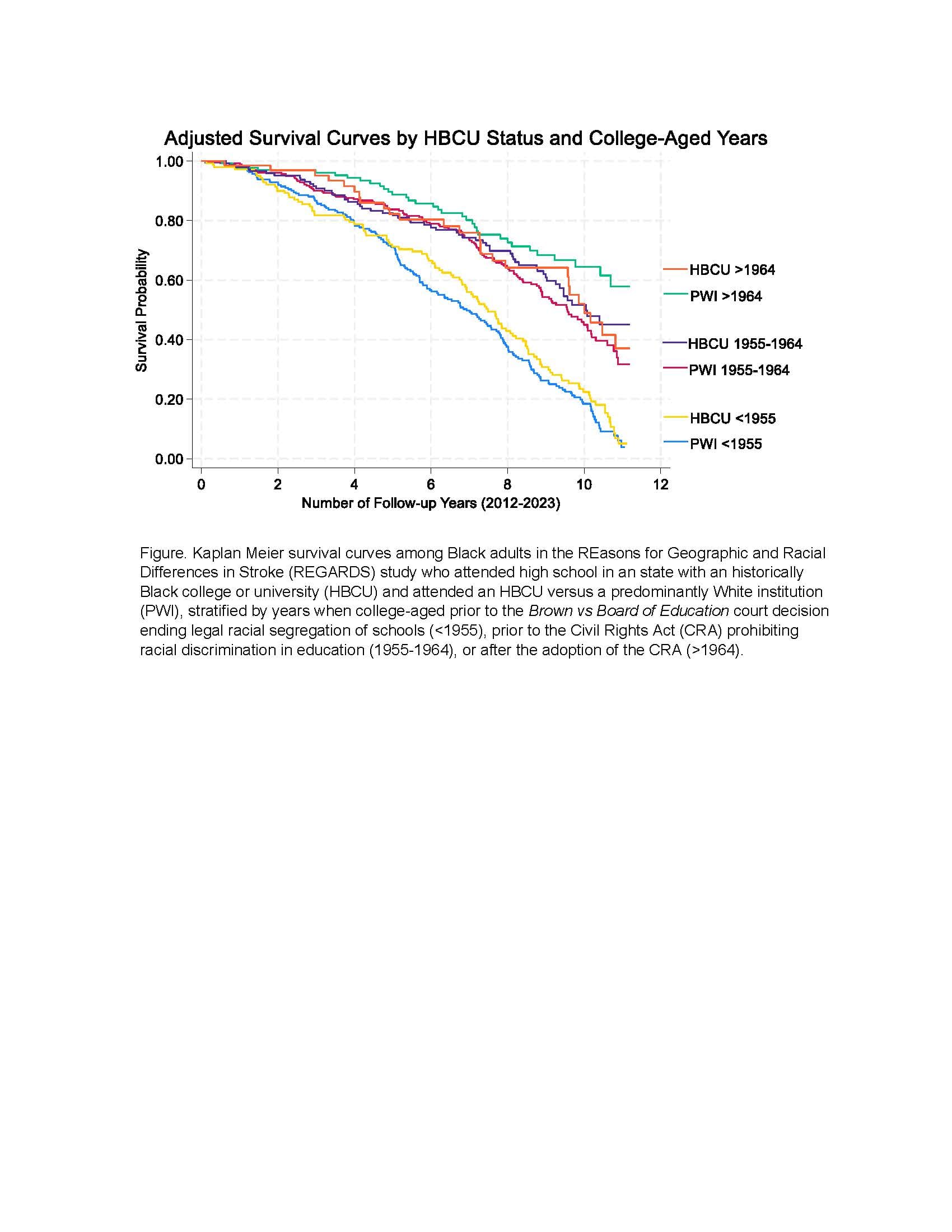
The REasons for Geographic and Racial Differences in Stroke (REGARDS) prospective study recruited Black and White US adults aged 45 and older during 2003-2007. The analytic sample included Black college-goers who attended high school in a state with an HBCU (N=1,960). In 2012, data collection was initiated on childhood, adult, and family factors. Participants retrospectively reported each college ever attended, which was classified as a PWI (reference) or HBCU. Every 6 months, interviews collected mortality information from next of kin or proxies. Adjusting for participant characteristics (e.g., age, gender) and early-life predictors (e.g., childhood health, school support), Cox proportional hazard models estimated adjusted mortality ratios (2012–2023) and effect modification by whether participants were college-aged before 1955 (during legal racial segregation), 1955-1964 (before the Civil Rights Act), or after 1964.
RESULTS
Mean age was 62 years (SD±8.2) and 35% attended an HBCU. HBCU versus PWI attendees had negligibly lower all-cause mortality (HR 0.99; CI 0.88, 1.12). Although CIs were wide, those college-aged during 1955-1964 had lower mortality (HR 0.87; CI 0.87, 1.06) but elevated mortality for those college-aged before 1955 (HR 1.03; CI 0.85, 1.24) and after 1964 (HR 1.46; CI 0.91, 2.33).
CONCLUSION
We found little evidence that HBCU attendance was associated with lower mortality yet could not rule out substantial protective or harmful effect modification by college-aged years. These results are inconsistent with prior findings related to other health outcomes.