Hospital costs of severe maternal morbidity across race/ethnicity and insurance status: a national serial cross-sectional study
Abstract
Objective: Medicaid covers over 40% of United States births and disproportionately serves racial minority groups who already face elevated obstetrical risks. Coverage gaps relative to private insurance may further exacerbate these adverse outcomes and their associated healthcare costs. We assessed the odds and hospital costs of severe maternal morbidity (SMM) at the intersection of race/ethnicity and insurance status.
Methods: We analyzed 23.5 million weighted obstetric deliveries from 2015-2022 using the National Inpatient Sample. Ten interaction terms were created to compare Medicaid versus private insurance across White, Black, Hispanic, Asian, and Native American groups. The 21 SMM complications were defined per CDC criteria using International Classification of Disease codes. Multivariable logistic regression and generalized linear models assessed SMM odds and associated hospital costs respectively, adjusting for a validated obstetric comorbidity score, discharge year/quarter, mode of delivery, and hospital region.
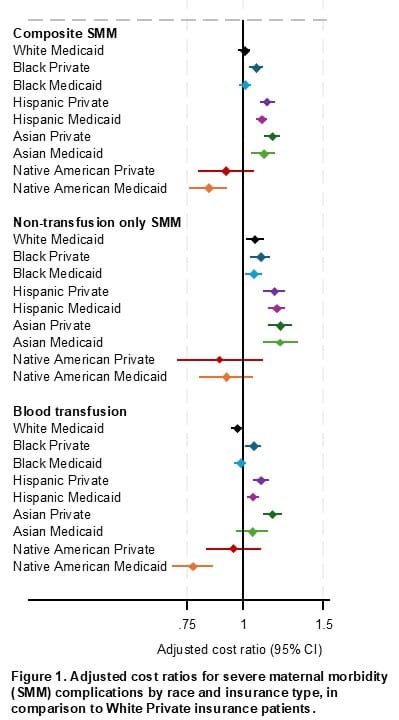
Results: Medicaid insured 43.8% of deliveries, with higher coverage among Native American (67.6%), Black (66.7%), and Hispanic (66.6%) patients compared to White (32.3%) and Asian (27.9%) patients. Adjusted odds of composite SMM were higher among all intersectional groups compared to privately insured White patients (p<0.001). Within each racial category, Medicaid was associated with higher odds of SMM. SMM-related costs were generally higher among Black, Hispanic, and Asian patients across insurance types whereas Native American Medicaid patients demonstrated significantly lower costs (Fig 1).
Conclusion: Racial disparities in SMM risk are significantly amplified for those with Medicaid, yet race appears to be the primary driver of the disproportionate financial burden. Addressing these inequities requires policy reform that targets both insurance coverage and the structural biases inherent to clinical care and resource allocation.