Clinical Preterm Delivery Phenotypes and Chronic Hypertension among Women in the Nurses’ Health Study II
Abstract
Preterm delivery (PTD) has been linked to elevated maternal cardiovascular disease. Yet mechanisms, such as chronic hypertension, underlying observed associations remain unclear due to limited investigation of clinical PTD phenotypes.
Leveraging data from 69,273 parous women in the Nurses’ Health Study II, we evaluated associations between lifetime PTD phenotype histories––spontaneous preterm labor (sPTL; n=1,775), preterm premature rupture of membranes (pPROM; n=1,037), medically indicated preterm delivery (miPTD; n=700), and/or nonphenotyped PTD (n=6,534)––and chronic hypertension up to 54 years since first birth. Cox proportional hazards models with time-varying exposures and covariates were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). We stratified estimates by time since first birth to identify potential periods of increased risk.
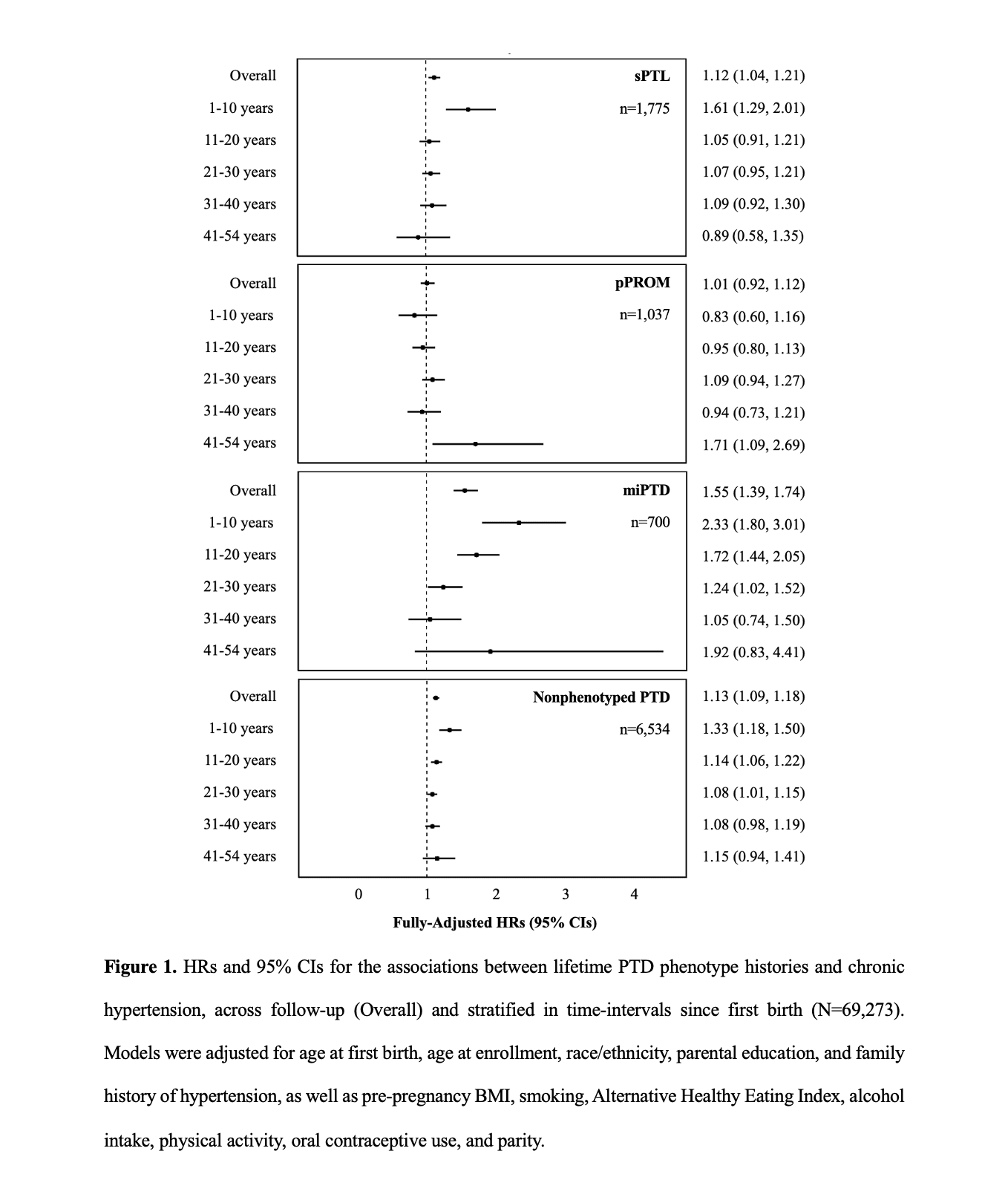
With a median follow-up of 29 years, we observed 27,376 (40%) cases of chronic hypertension. Lifetime histories of miPTD, sPTL, and nonphenotyped PTD were associated with 55% (HR 1.55; CI 1.39, 1.74), 12% (HR 1.12; CI 1.04, 1.21), and 13% (HR 1.13; CI 1.09, 1.18) increased rates of chronic hypertension, respectively, as compared to pregnancy histories uncomplicated by each phenotype. Adjustment for hypertensive disorders of pregnancy attenuated estimates for miPTD (HR 1.22; CI 1.09, 1.37), suggesting much of the risk associated with miPTD is driven by preeclampsia and gestational hypertension. Rates of chronic hypertension were highest in the first 10 years for miPTD (HR 2.33; CI 1.80, 3.01), sPTL (HR 1.61; CI 1.29, 2.01), and nonphenotyped PTD (HR 1.33; CI 1.18, 1.50). For pPROM, elevated risk of chronic hypertension emerged only after 40 years (HR 1.71; CI 1.09, 2.69).
Rates of chronic hypertension differed across clinical PTD phenotypes. Women with a lifetime history of miPTD were at greatest risk, especially during the first 10 years postpartum, indicating a critical window for screening and intervention.