Perinatal & Pediatric
Fetal and infant death among mothers with intellectual and developmental disabilities in California, 2007-2021. Catherine Psaras* Catherine Psaras Psaras Psaras University of California, San Diego
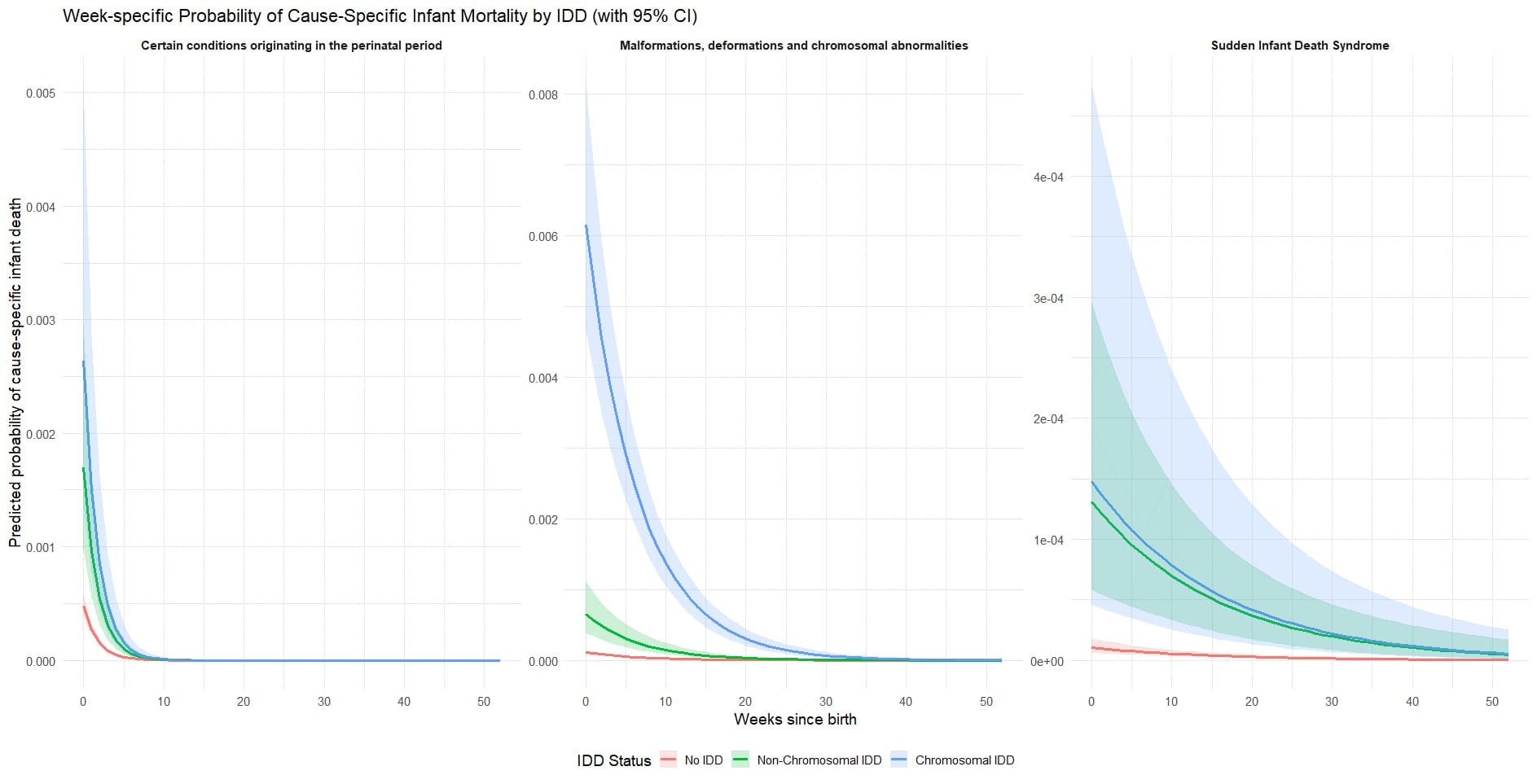
Mothers with intellectual and developmental disabilities (IDD) experience disparities in pregnancy outcomes, yet heterogeneity across IDD subtypes is poorly understood. We quantified associations between maternal IDD subtype and fetal and infant death. Using California vital statistics birth and fetal/infant death records linked to hospital discharge data from the Study of Mothers and Infants (2007-2021), we conducted a retrospective cohort study. Maternal IDD was identified via hospital discharge codes and classified as chromosomal (e.g., trisomies, Fragile X) or non-chromosomal (e.g., intellectual disability, autism, cerebral palsy). Pooled logistic regression estimated ORs for fetal death, infant death, and cause-specific infant death, adjusting for maternal age and delivery year. Infant death models used stabilized inverse probability of selection weights to account for differential fetal loss. Compared with mothers without IDD, fetal death odds were elevated for non-chromosomal IDD (OR: 3.98; 95% CI: 3.53-4.48) and higher for chromosomal IDD (OR: 16.31; 95% CI: 14.92-17.38). Infant death showed similar patterns (non-chromosomal IDD OR: 5.99; 95% CI: 5.44-6.58; chromosomal IDD OR: 22.79; 95% CI: 21.05-24.67). The largest differences were for deaths due to infant congenital malformations, deformations, and chromosomal differences, particularly among maternal chromosomal IDD (OR: 54.33; 95% CI: 40.04-73.71). Both IDD groups also had elevated risks of death due to sudden infant death syndrome and conditions originating in the perinatal period compared to mothers without IDD (see figure). Mediation analyses showed that maternal comorbidities accounted for only a small proportion of fetal death risk (9%; 95% CI: 3%-17%), while maternal comorbidities and adverse birth outcomes accounted for a substantially larger share of infant death risk (33%; 95% CI: 27%-40%), primarily through preterm birth (<37 weeks).