Etiology-specific population attributable fractions for Acute Febrile Illness in the Peruvian Amazon: Findings from the first three years of the RIVERA case-control study, 2021 – 2024
Abstract
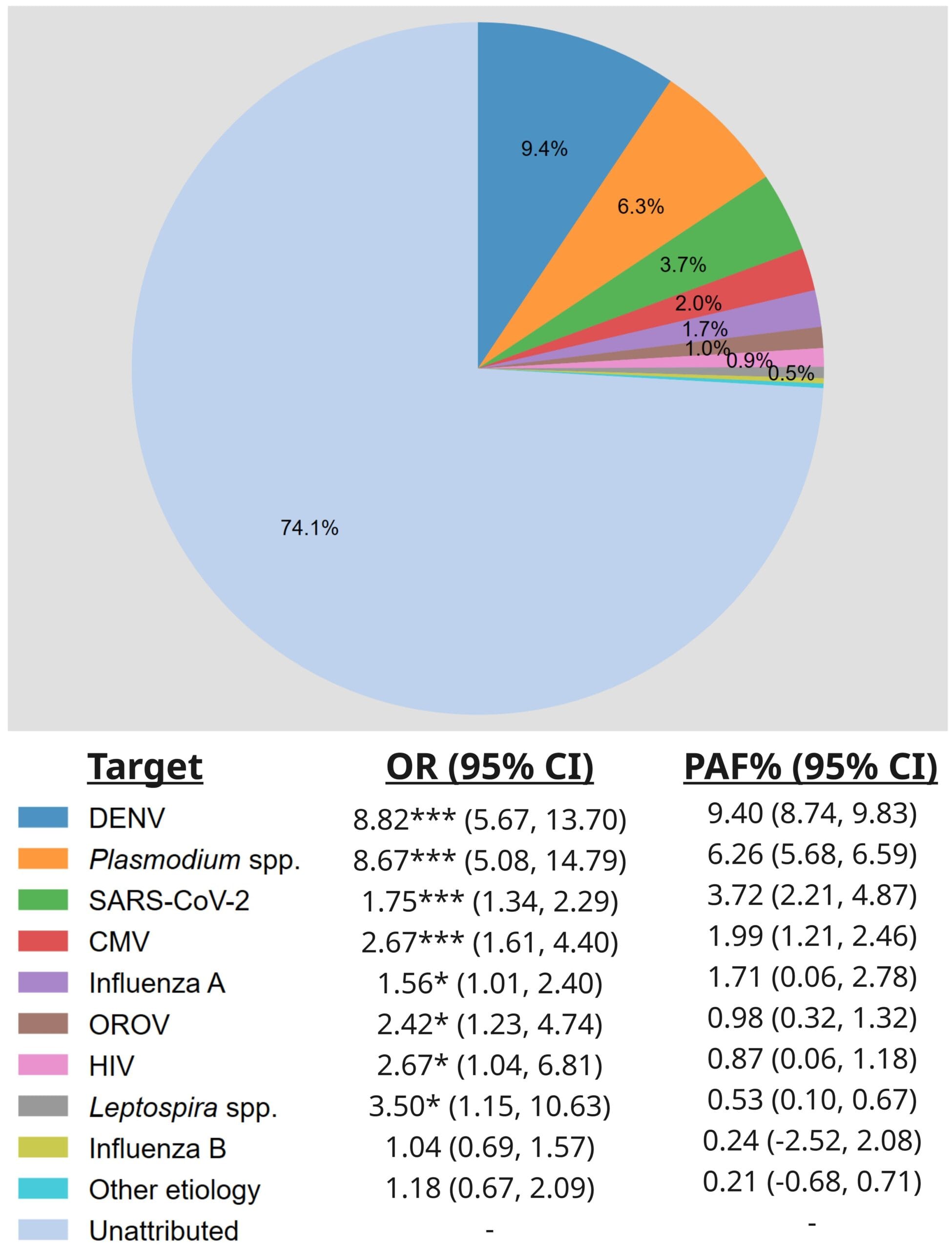
Acute febrile illness (AFI) is a major cause of primary care-seeking in the Peruvian Amazon and across the Tropics and caused by a range of bacterial, viral, and parasitic pathogens. Due to diagnostic limitations AFI cases are seldom attributed to specific etiologies, leading to a large diagnostic gap. RIVERA is a health facility-based prospective case-control surveillance study conducted in and around the Peruvian city of Iquitos. 1,898 AFI cases were enrolled and matched 1:1 with afebrile controls. Baseline and follow-up (3-4 weeks later) questionnaires were administered, and blood, saliva, and nasal swab samples collected and tested for 36 pathogen targets by PCR. Clinical characteristics, risk factors, and pathogen detections were compared using odds ratios (ORs) and population attributable fractions (PAFs) from univariate conditional logistic regression models. Statistically and clinically significant variables were included in a final, multivariable models, from which adjusted ORs (aORs) and PAFs (aPAFs) were derived. AFI cases had increased odds of recent travel by river (OR=7.72 [95% CI: 4.99, 11.95]), or other mode (4.68 [1.83, 11.94]), and of reporting ticks (2.58 [1.61, 4.14]) but not fleas (0.82 [0.49, 1.36]) on their bodies, and bats (1.65 [1.29, 2.11]) but not rats (1.14 [0.97, 1.34]) in their homes. The most prevalent pathogen in the study population was SARS-CoV-2 followed by dengue virus (DENV), Plasmodium, influenzas B and A, cytomegalovirus (CMV) and Oropouche virus (OROV), all of which were detected in asymptomatic controls as well as AFI cases. Over a third of the AFI burden in this setting is attributable to just five pathogens – DENV, OROV, SARS-CoV-2, Plasmodium spp. and CMV – after adjustment for temporal variation, background asymptomatic carriage and various comorbidities, risk factors and confounders. A large fraction of the AFI burden remains unattributed despite the extensive, contextually tailored panel of pathogen tested.