Application of Disease Risk Scores to Obtain Individualized Estimates of Ibuprofen Associated Acute Kidney Injury in Hospitalized Patients
Abstract
Background: Non-steroidal anti-inflammatory drugs (NSAID) are key opioid-sparing options in hospitals but may increase acute kidney injury (AKI) risk. Prior studies evaluated heterogeneous treatment effects (HTE) by individual characteristics (e.g., age, kidney function), but do not capture how multiple factors combine to modify treatment effects. Disease risk score (DRS) approaches can address this limitation by summarizing multiple AKI risk factors into a single measure.
Objective: To determine whether NSAID effects on AKI vary by baseline AKI risk.
Methods: We conducted an active comparator cohort study of patients hospitalized in the University of Pennsylvania Health System treated with the NSAID ibuprofen versus those treated with oxycodone. Using split-sample estimation, we estimated an AKI DRS with logistic regression on 68 baseline covariates in a randomly selected half of oxycodone patients (training set). Using this model, we estimated DRS on the remaining patients and stratified patients into DRS quartiles. We estimated inverse probability of treatment weights within each DRS stratum and estimated stratum-specific incidence rate differences (IRD). We also estimated treatment effects as a continuous function of the DRS.
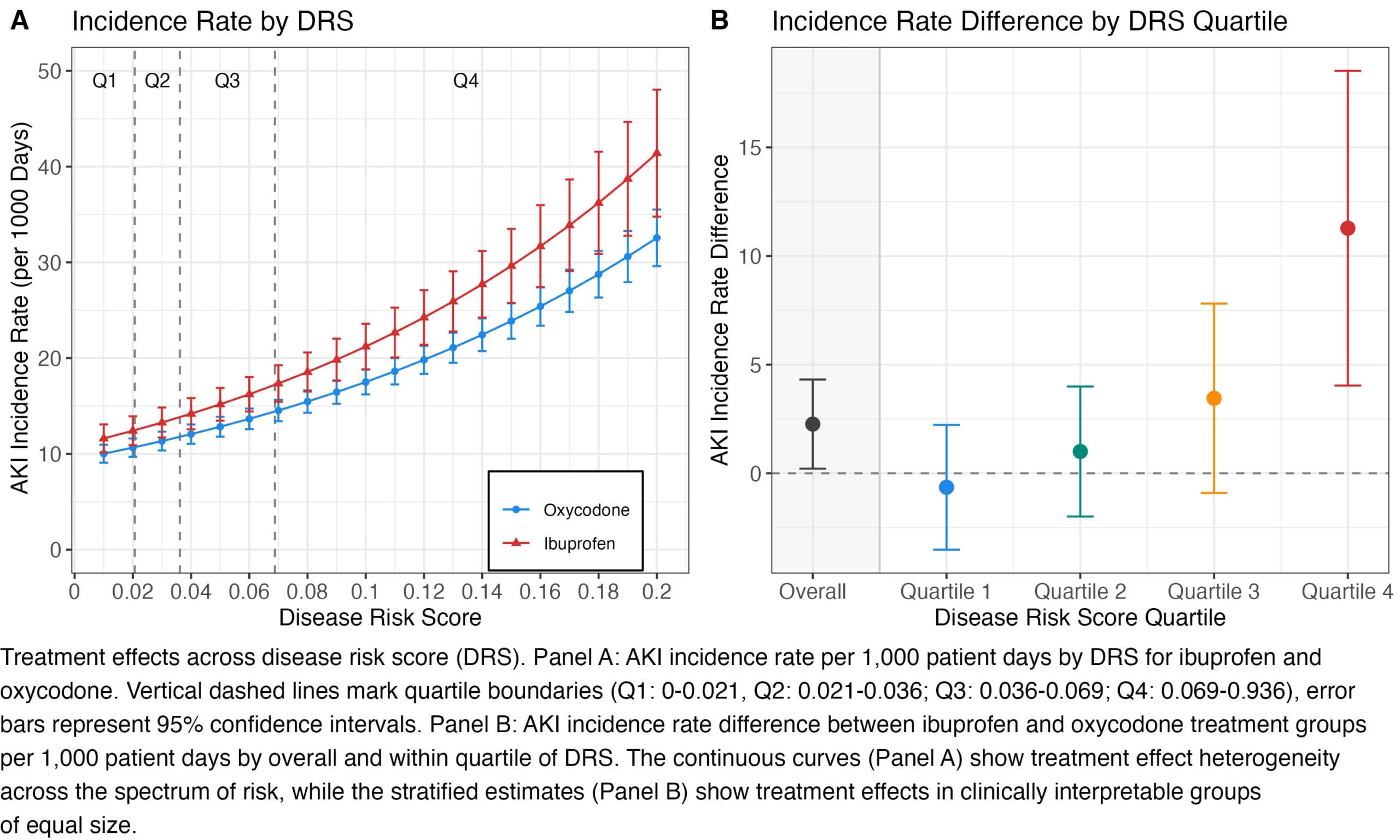
Results: The DRS development set included 36,171 patients who experienced 2,243 AKI events. The outcome analysis included 42,485 patients (ibuprofen = 6,313, oxycodone = 36,172) with 2,556 AKI events. The overall adjusted AKI incidence rate was 16.41 and 14.14 per 1000 days in the ibuprofen and oxycodone groups, respectively (IRD = 2.26 per 1000 days, 95% CI [0.21, 4.31]). The IRD was 11.28 per 1000 days (95% CI [4.04, 18.52]) in the highest DRS quartile and -0.64 per 1000 days (95% CI [-3.52, 2.23]) in the lowest DRS quartile.
Conclusion: Our results suggest the effect of ibuprofen on AKI varies >10-fold across levels of baseline AKI risk. DRS stratification may be a useful tool for individualized NSAID treatment in hospitalized patients.