Toward scalable and equitable risk prediction for internalizing disorders in adolescence
Abstract
Adolescence is the peak period for onset of internalizing disorders (e.g. anxiety, depression) and a critical intervention window. Scalable intervention requires prospectively identifying high-risk youth using information feasible to obtain in clinical care. Progress in risk prediction is slowed by disciplinary silos, minimal attention to feasibility of collecting predictors in clinical settings, scarce evaluation of algorithmic fairness, and arbitrary dichotomizations of continuous psychiatric phenomena.
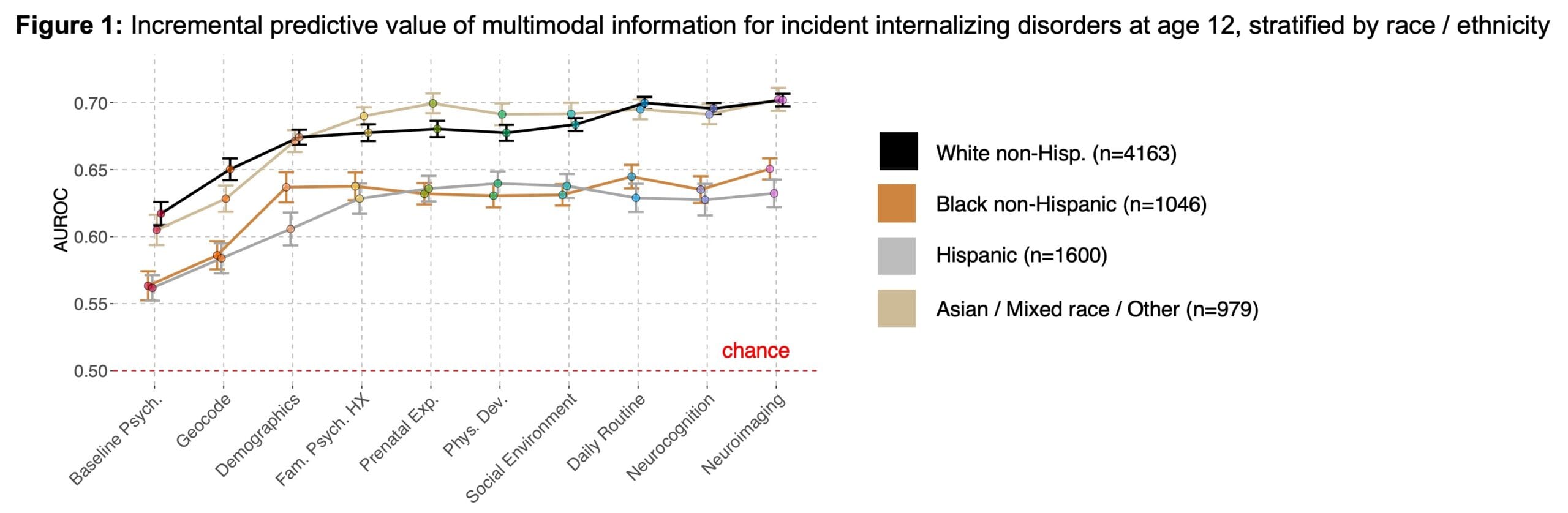
We use multimodal data collected at ages 9-10 from ~10k participants in the Adolescent Brain and Cognitive Development Study to predict internalizing symptom severity by ages 14-15. >300 predictors are grouped into “layers” and ordered by anticipated feasibility: baseline psychopathology, neighborhood features, familial psychiatric history, prenatal exposures, anthropometrics, social environment, daily routine, cognition, hormones, genomics and neuroimaging. Machine‑learning models (gradient-boosted trees, random forest, LASSO) are fit with nested cross-validation, adding layers stepwise to quantify incremental gains from higher-cost modalities. To evaluate fairness, we test whether overall performance and the added value of costly layers differ by racial identity. Initial analyses using a binary internalizing outcome at age 12 (Fig. 1) show modest discrimination (AUROC ~ 0.55-0.7), limited improvement from layers beyond familial history, and lower performance for Black and Hispanic youth than White youth. Ongoing work extends these models to a continuous symptom outcome at ages 14-15, when incidence peaks, and incorporates hormonal and genomic predictors. Updated results will be presented.
Rather than proposing a deployable risk calculator, this work delineates practical limits of prediction, clarifies when high-cost modalities meaningfully improve performance, and informs cautious development of scalable, equitable risk-stratification tools in youth mental health.