Individualized Growth Assessment Compared to Conventional Growth Charts for Detecting Growth-Related Morbidity
Abstract
Individualized growth assessment (IGA) evaluates growth adequacy using each fetus as its own control. It is unclear whether IGA improves the ability to distinguish pathological fetal growth from constitutional small or large-for-gestational-age (SGA or LGA).
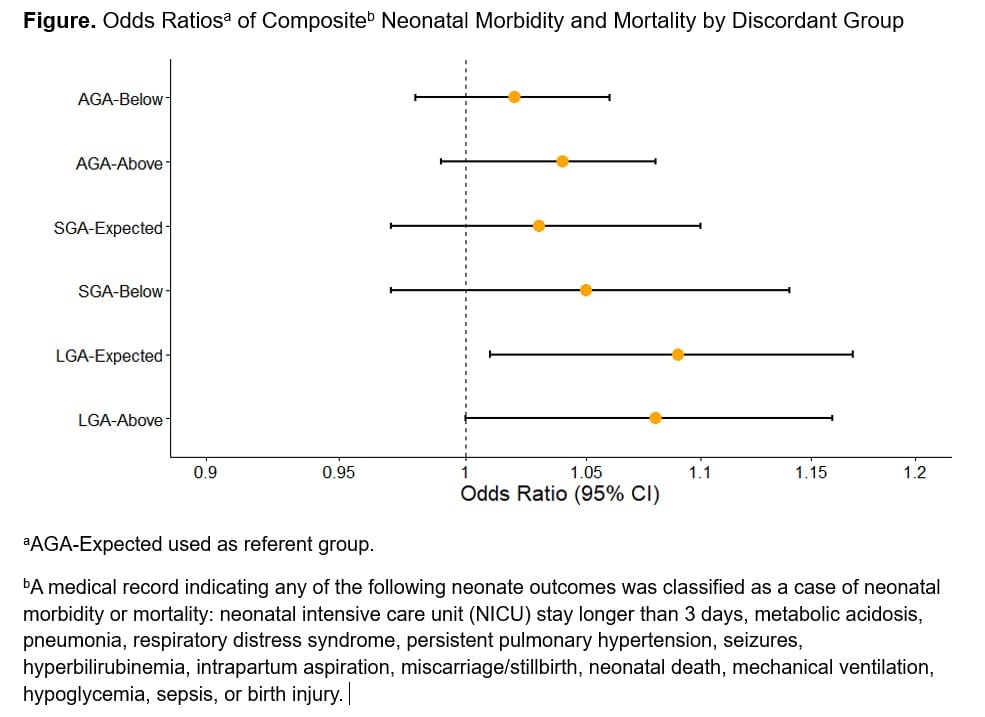
In a prospective cohort of 2,310 women with fetal measurements at up to 5 visits, we calculated estimated fetal weight (EFW) from 5,915 third trimester (3T) sonograms. EFW was categorized at each 3T scan by 2 methods: 1st as SGA, <10th; AGA, 10th-90th; or LGA, >90th percentile using NICHD unified growth charts; and 2nd by IGA which uses two second trimester scans and the Rossavik Growth Model to predict 3T growth potential and categorized each 3T scan as at, below, or above, expected growth potential. We compared categorization concordance, and predictive accuracy for composite neonatal morbidity/mortality (Fig legend). Logistic regression via GEE calculated odds of neonatal morbidity by discordant group (reference AGA-expected concordant group).
4,761 scans (80.5%) were categorized as AGA, 9.3% SGA, and 10.2% LGA using NICHD growth charts and 81.4%, 7.4%, and 11.2% at, below, or above expected using IGA. Among AGA, neonatal morbidity was 9.6% vs. 5.6% (p= 0.005) for above vs. expected by IGA, and 6.4% vs. 5.6% (p= 0.62) for below vs. expected. Among SGA, 9.2% vs. 6.6% (p= 0.26) for below vs. expected by IGA. Among LGA 8.8% vs. 10.3% (p= 0.54) for above vs. expected by IGA. Risk of composite neonatal morbidity/mortality was increased only for LGA-Expected, although LGA-Above had similar magnitude, but was statistically insignificant (Fig).
Evidence suggests IGA may improve detection of growth-related morbidity among smaller fetuses, but there was no improvement in our low-risk sample. Among larger fetuses, IGA may be less effective, as large size is an independent morbidity risk factor, e.g. birth injuries. Future comparisons should focus on high-risk pregnancies that may benefit most from improved detection.