Real-World Adherence to Annual Lung Cancer Screening with Low-Dose CT Accounting for Competing Risks
Abstract
Background:
Annual lung cancer screening (LCS) with low-dose computed tomography (LDCT) reduces lung cancer mortality among high-risk individuals, but the effectiveness of this intervention depends upon adherence to annual screening. We quantified and described real-world adherence to annual LCS with LDCT among Medicare beneficiaries.
Methods:
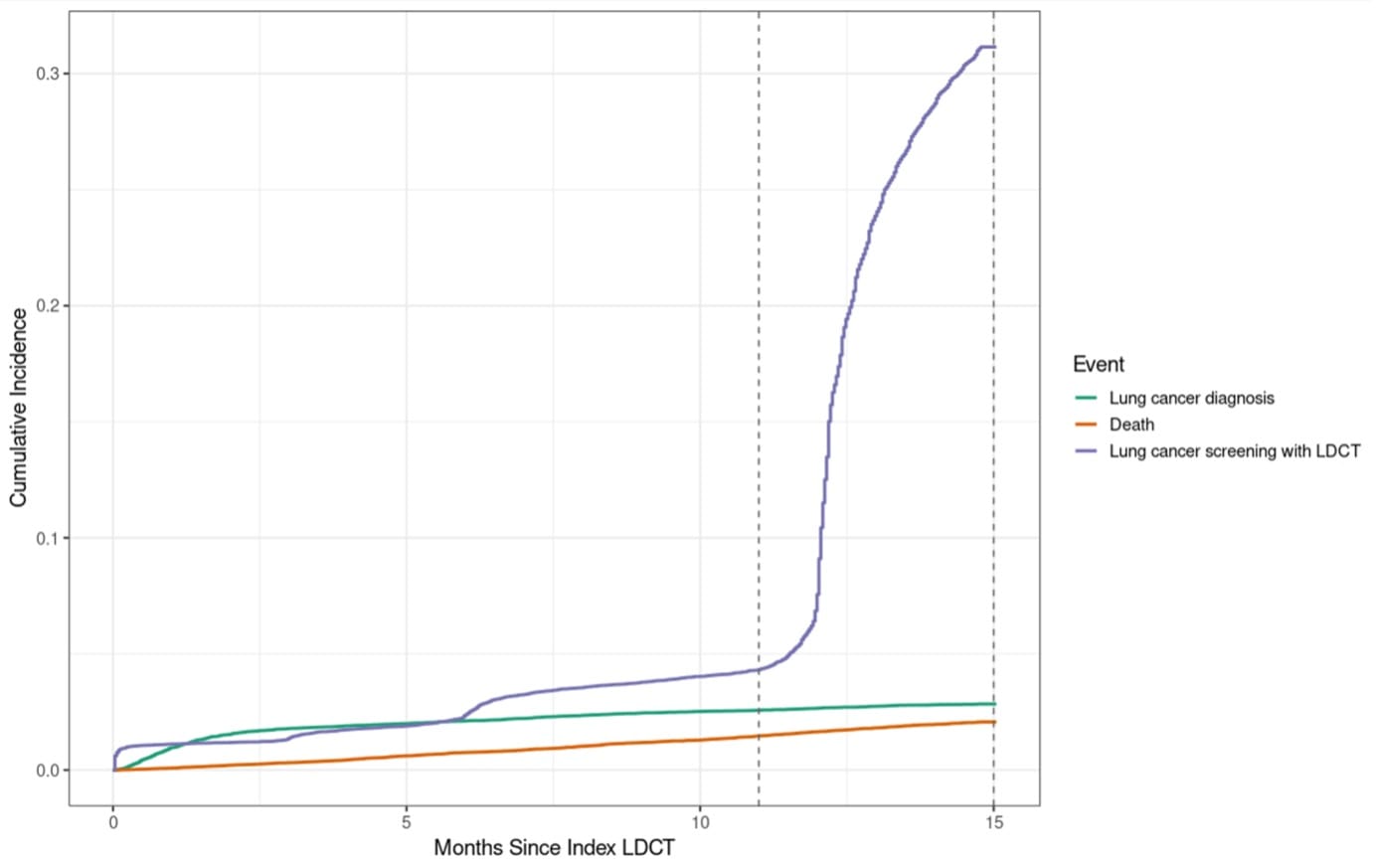
We conducted a retrospective cohort study of individuals, aged ≥66 years, who received a first LCS with LDCT between 2015 and 2019, and had no prior history of lung cancer, using Medicare fee-for-service claims. Annual adherence was defined as receipt of a subsequent LDCT screening within 11 to 15 months of the first screen. We estimated cumulative incidence functions (CIFs) using Aalen-Johansen estimator, treating lung cancer diagnosis and death as competing events. CIFs were estimated overall and stratified by age, sex, race and ethnicity, comorbidity index, and frailty index. We reported the cumulative incidence from 11 to 15 months, as this represents a reasonable window for determining adherence to annual LCS. We estimated 95% confidence intervals using non-parametric bootstraps with 500 replicates.
Results:
Among 54,978 patients with an initial LDCT claim, the cumulative incidence of subsequent LCS was 4.3% (95% CI: 4.1-4.5%) at 11 months, and 31.1% (95% CI: 30.7-31.6%) at 15 months, with an annual adherence of 26.8% (95% CI: 26.3-27.3%) between 11 and 15 months. Adherence to LCS was higher among those who were younger, white, less frail, and had lower comorbidity burden. The cumulative incidences of lung cancer and death were 2.1% (95% CI: 2.0-2.2%) and 2.9% (95% CI: 2.7-3.0%), respectively.
Conclusions:
Real-world adherence to annual lung cancer screening with LDCT remains suboptimal among Medicare beneficiaries, with fewer than one-third completing subsequent screening within 15 months. These findings highlight a gap in screening implementation that may limit its effectiveness at the individual and population-levels.