Coronary Artery Calcium and Incident Atherosclerotic Cardiovascular Disease: An Application of Generalized Heterogeneous Treatment Effect (HTE) Approach
Abstract
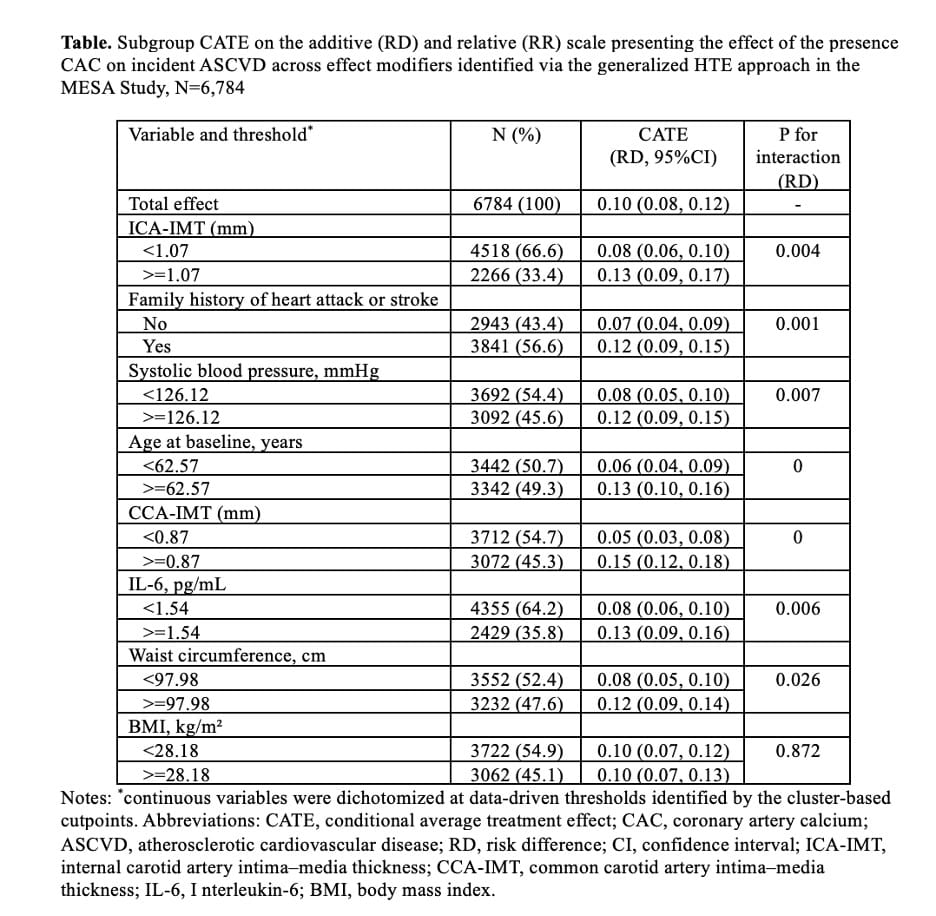
Coronary artery calcium (CAC) is a strong marker of subclinical atherosclerosis, but its prognostic value for atherosclerotic cardiovascular disease (ASCVD) may differ across individual background characteristics. Our objective was to identify baseline factors that meaningfully modify the CAC–ASCVD association and quantify subgroup-specific effects using a generalized heterogeneous treatment effect (HTE) framework. We analyzed 6,784 MESA participants aged 45–84 years free of clinical cardiovascular disease at baseline (2000–2002) and were prospectively followed through 2015. CAC presence was defined by Agatston score >0. Incident ASCVD cases included coronary heart disease, stroke or transient ischemic attack, peripheral vascular disease, and ASCVD-related death. We applied a generalized HTE approach based on parametric g-computation, incorporating stabilized inverse probability of treatment weighting to adjust for baseline confounding and LASSO-regularized logistic models to reduce overfitting and select potential effect modifiers. Counterfactual risk prediction was used to estimate individualized and subgroup-specific conditional average treatment effects (CATEs) on the risk difference scale. A hierarchical clustering approach was then used to identify effect-modifying subgroups. CAC was present in 3,383 participants (49.9%) at baseline, and 1,028 ASCVD events occurred over 15 years. CAC presence was associated with higher ASCVD risk (risk difference 0.10; 95% CI, 0.08–0.12). Greater CAC-attributable excess risk was observed among participants with higher carotid intima-media thickness, older age, higher systolic blood pressure, elevated interleukin-6, larger waist circumference, and a positive family history of cardiovascular disease compared with their counterparts (Table). The association between CAC and ASCVD risk is heterogeneous, with stronger effects among individuals with vascular, inflammatory, and metabolic vulnerability. These findings support more selective, context-informed use of CAC testing to guide primary prevention.