When high risk is not one category: Transportability of 17 alpha-hydroxyprogesterone caproate trial results in preterm delivery
Abstract
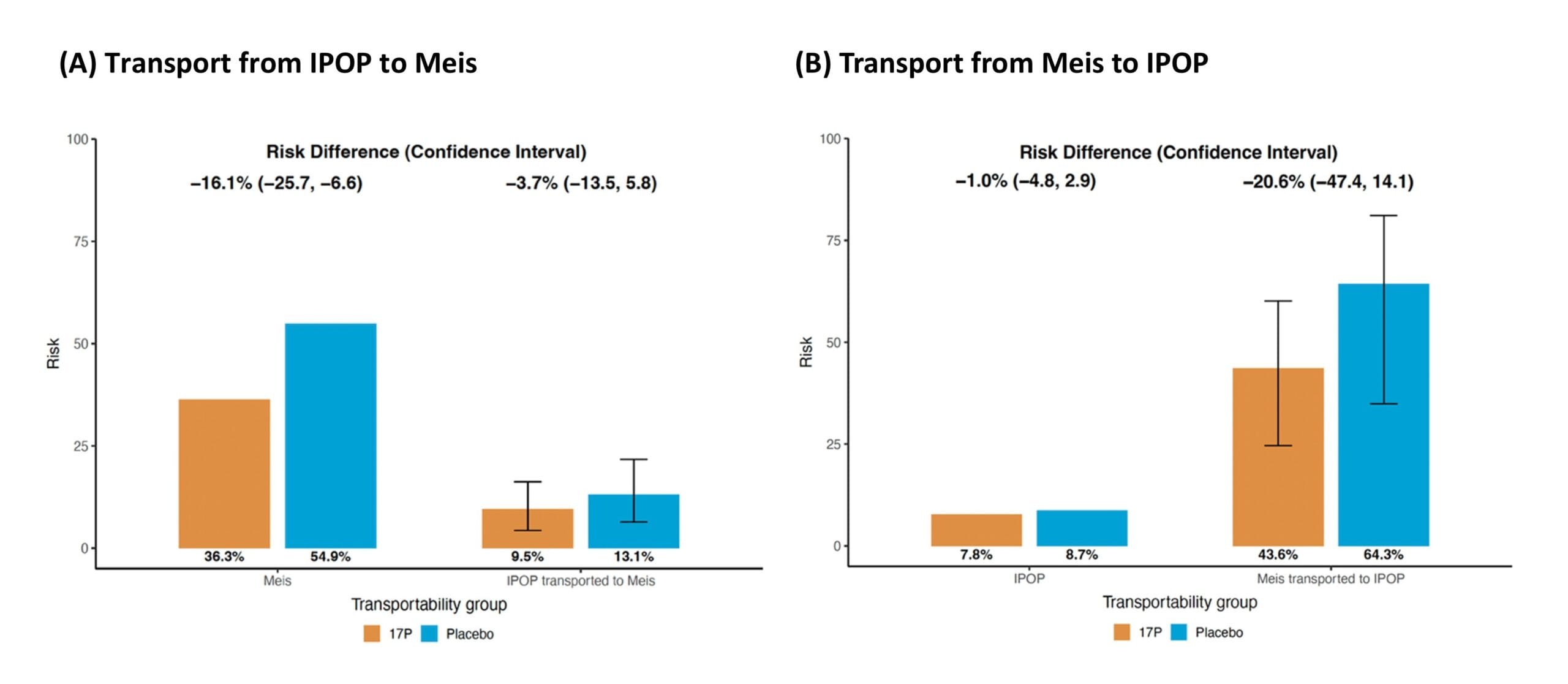
Background: The 2003 Meis trial found that 17α-hydroxyprogesterone caproate (17OHP-C) reduced recurrent preterm birth among individuals with a prior spontaneous preterm delivery (RD, −18.6%; 95% CI, −28.2% to −9.1%). In contrast, the 2021 IPOP trial found no benefit of 17OHP-C for preventing preterm birth among pregnant individuals living with HIV without a history of preterm birth (RD, −1.0%; 95% CI, −4.8% to 2.9%). Although both populations are considered at high risk for preterm birth, the trials differed not only in eligibility pathways but also in age, education, and other sociodemographic factors. These conflicting findings have raised questions about whether differences in population characteristics may explain the inconsistency in 17OHP-C’s effectiveness across high-risk groups.
Methods: We conducted bidirectional transportability analyses, transporting treatment effects from Meis to IPOP and from IPOP to Meis, using individual participant data from both trials. In the original trials, weekly intramuscular injections of 17OHP-C or placebo were administered. The primary outcome in this study was preterm delivery before 37 weeks’ gestation. We used doubly robust estimators combining outcome modeling with inverse odds of trial selection weighting to transport treatment effects between trials while accounting for differences in baseline covariates.
Results: Transporting the Meis results to the IPOP population yielded an RD of −20.6% (95% CI, −47.4% to 14.1%), indicating a more protective effect than the original IPOP estimate, although with a wide CI overlapping the IPOP result. Transporting the IPOP results to the Meis population produced an RD of −3.7% (95% CI, −13.5% to 5.8%), moving closer to but not aligning with the Meis estimate. Restricting Meis participants to those with documented infections during pregnancy attenuated the result (RD, −8.0%; 95% CI, −24.3% to 8.4%) and more closely matched the IPOP findings.
Discussion: These findings indicate that differences in measured baseline characteristics did not explain the inconsistency between trials. The effectiveness of 17OHP-C may vary by underlying biological pathways and may not generalize across distinct high-risk populations.