From Guideline to Practice: A Quasi-Experimental Evaluation of Hypertensive Disorders of Pregnancy Following the ACOG Low-Dose Aspirin Recommendation in Pregnancies With Pregestational Diabetes
Abstract
Background: The American College of Obstetricians and Gynecologists (ACOG) recommends low-dose aspirin (LDA) for the prevention of preeclampsia among high-risk pregnancies, including those complicated by pregestational diabetes (PGD). However, recent randomized controlled trials (RCTs) have questioned the efficacy of LDA in this population. We leveraged the 2016 ACOG guideline update as a natural experiment to evaluate the real-world impact of guideline adoption on maternal outcomes among pregnancies with PGD.
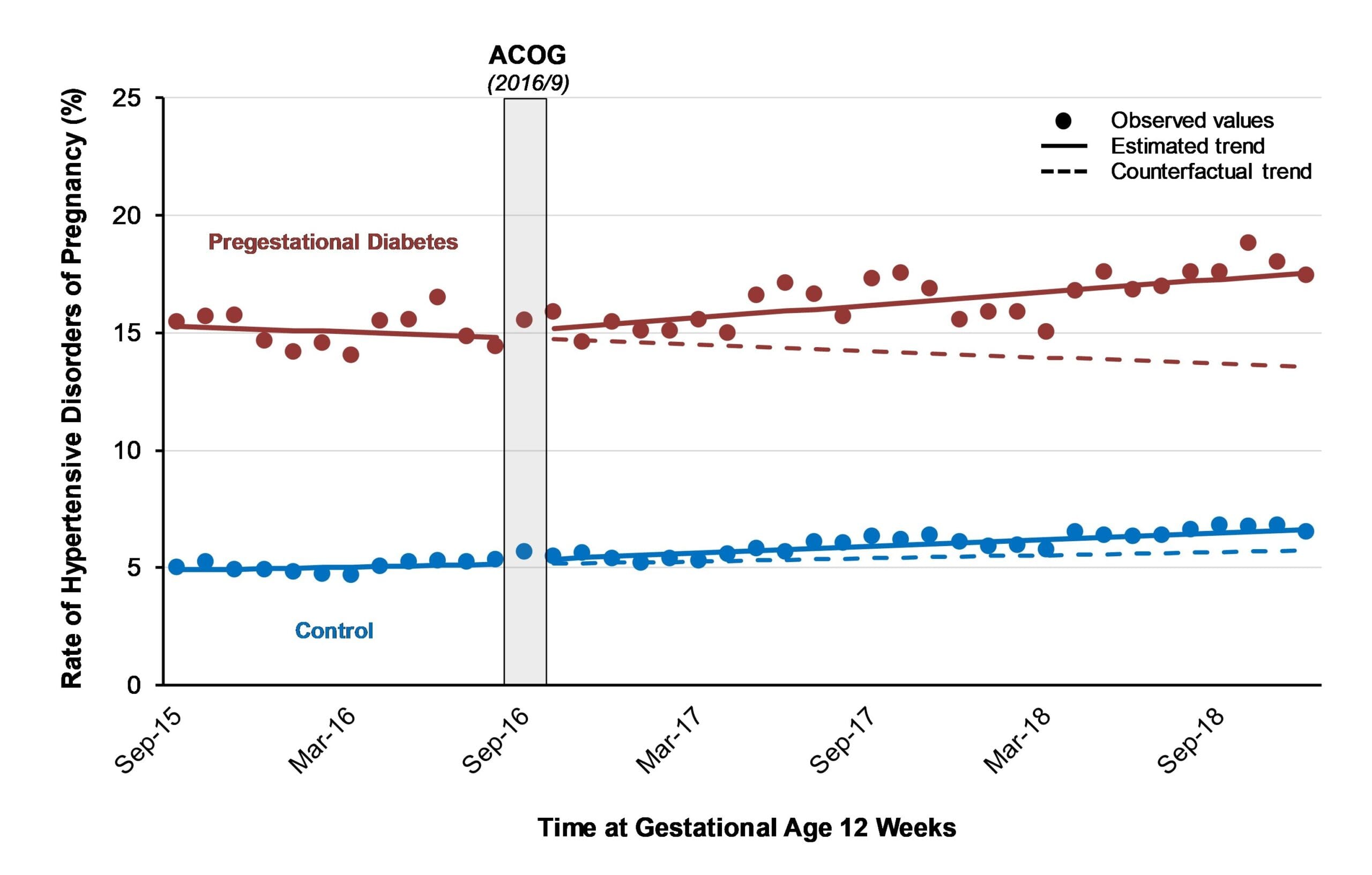
Methods: We conducted a controlled interrupted time-series (CITS) analysis using US National Vital Statistics System birth certificate data. Time was indexed by calendar month at gestational age 12 weeks, spanning September 2015 through December 2018, with the September 2016 ACOG guideline update treated as the intervention point. Pregnancies with PGD were compared with a low-risk control group defined as nulliparous individuals younger than 35 years with a normal pre-pregnancy body mass index and no history of PGD, chronic hypertension, or assisted reproductive technology use. This control group was used to address potential confounding from concurrent interventions or underlying temporal trends. The primary outcome was hypertensive disorders of pregnancy (HDP) recorded on the birth certificate, defined as a composite of gestational hypertension and preeclampsia. Segmented regression models were used to estimate between-group differences in immediate level changes and post-guideline trend changes on the absolute risk scale.
Results: The analysis included 75,123 pregnancies with PGD and 993,450 low-risk control pregnancies. The CITS analysis showed no evidence of a between-group, guideline-associated change in HDP, with an estimated immediate level change of 0.18% (95% CI, −1.13 to 1.48) and no differential post-guideline trend change (0.12% per month; 95% CI, −0.06 to 0.30).
Conclusion: In this population-based CITS analysis, real-world uptake of the 2016 ACOG recommendation for LDA was not associated with a reduction in HDP, including preeclampsia, among pregnancies with PGD. These findings are consistent with recent RCT evidence and underscore the need for further research to evaluate the effectiveness of LDA and alternative preventive strategies in this population.