Precision Medicine Approach to Elective Induction Decisions: Secondary Analysis of A Randomized Trial of Induction Versus Expectant Management (ARRIVE)
Abstract
Elective induction at 39 weeks reduces cesarean risk among low-risk pregnancies, but outcome heterogeneity may be masked. We evaluated whether individualized treatment rules could improve outcomes.
We analyzed ARRIVE trial data (N=6,106 low-risk nulliparas randomized at 38 weeks’ gestation to undergo either elective induction at 39 weeks or expectant management) using intention-to-treat. Baseline covariates included maternal age, height, weight, BMI, cervical dilation, Bishop score, assisted conception, substance use, marital status, employment, insurance, prior pregnancy loss, and fetal anomaly. We estimated individualized treatment effects on cesarean delivery and a perinatal (fetal/neonatal) morbidity/mortality composite using causal forests. Three individualized policies were defined: (A) induce if lower cesarean risk for induction versus expectant management, (B) induce if lower perinatal composite risk, and (C) induce if lower cesarean risk without increased perinatal risk. Expected risks under each policy, including universal induction and expectant management, were estimated via augmented inverse-probability-weighting with 5-fold cross-fitted SuperLearner. Missing data were replaced by 20 imputations using chained equations.
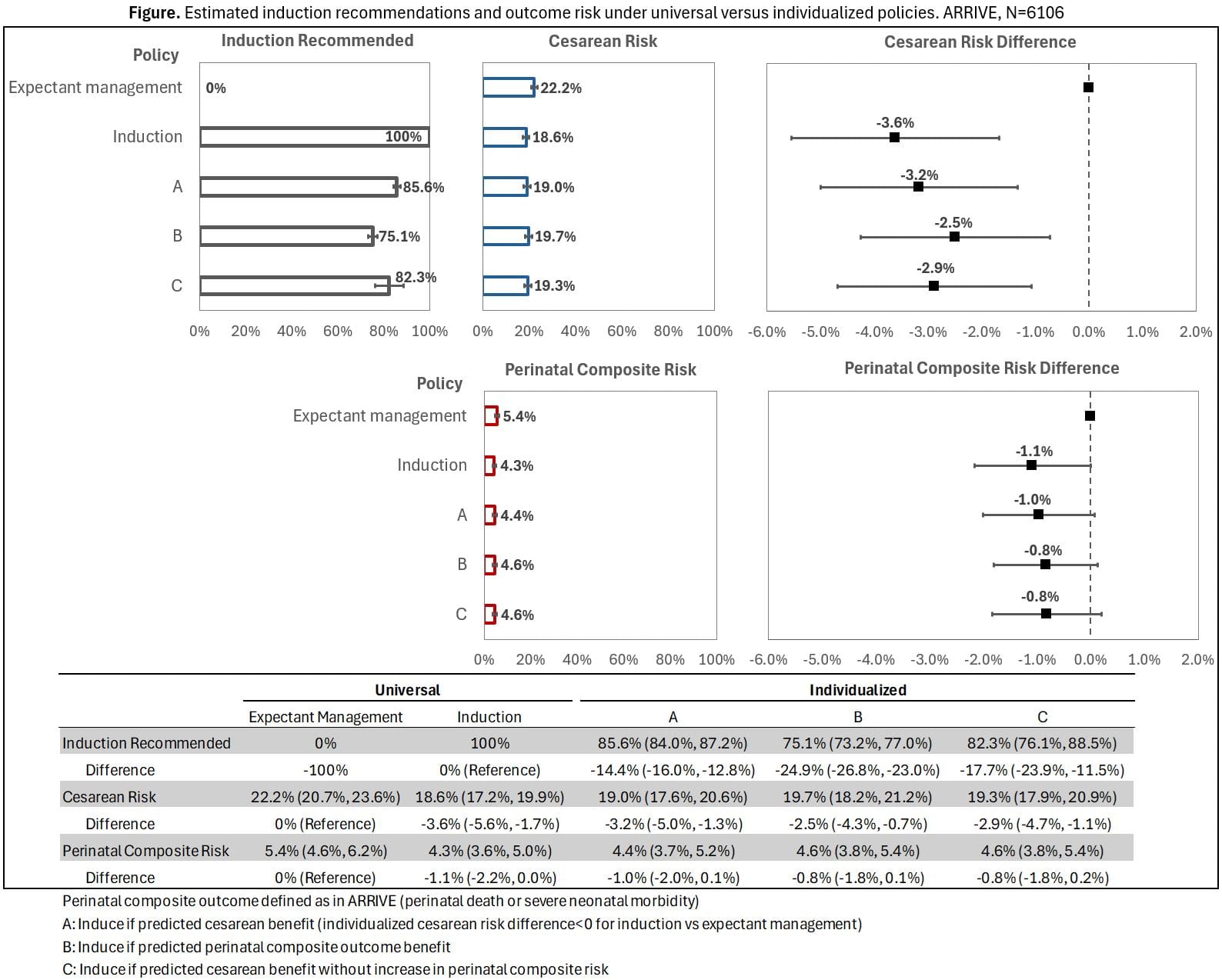
Compared to universal expectant management, universal induction had 18.6% cesarean (RD: −3.6% [95% CI: -5.6, -1.7]) and 4.3% perinatal composite risk (RD: -1.1% [-2.2, 0.0]). Individualized policies (A-C) recommended induction for 75.1-85.6% of participants, achieving 19.0-19.7% cesarean and 4.4-4.6% perinatal risk (Figure).
In ARRIVE, universal induction achieved the lowest cesarean risk, but individualized policies reduced inductions by 14–25 percentage points while maintaining lower cesarean and perinatal risks than universal expectant management. Individualized strategies may support patient-centered decision-making by identifying patients for whom elective induction is unlikely to provide cesarean or perinatal risk reduction.