Generalizing per protocol estimates of HIV treatment from the ACTG A5202 trial.
Abstract
Introduction: In the presence of non-adherence per-protocol estimators are attractive alternatives to intent-to-treat (ITT) estimators, because they can account for non-adherence to assigned treatment. Per protocol analyses typically only estimate treatment effects in the study sample, rather than generalize to a given target population. Our objective was to estimate HIV treatment efficacy in the ACTG A5202 trial generalized to the target population of newly infected HIV persons in the United States in 2008-2009 under multiple definitions of protocol adherence.
Methods: A reanalysis of ACTG A5202 evaluating Tenofovir/Emtricitabine (TDF/FTC) versus Abacavir/Lamivudine (ABC/3TC). Protocols were defined as ITT, and 1 dose missed and 2 dose missed protocols, which censored after missing 1 and 2 doses, respectively. We evaluated the composite risk of viral failure and death at 48 and 96 weeks. Inverse probability weighting was used to evaluate per protocol estimates. CDC data from 2008-2009 and inverse odds of sampling weights were used to generalize to the US population with incident HIV. Weighted Kaplan-Meier estimators were used to estimate risk.
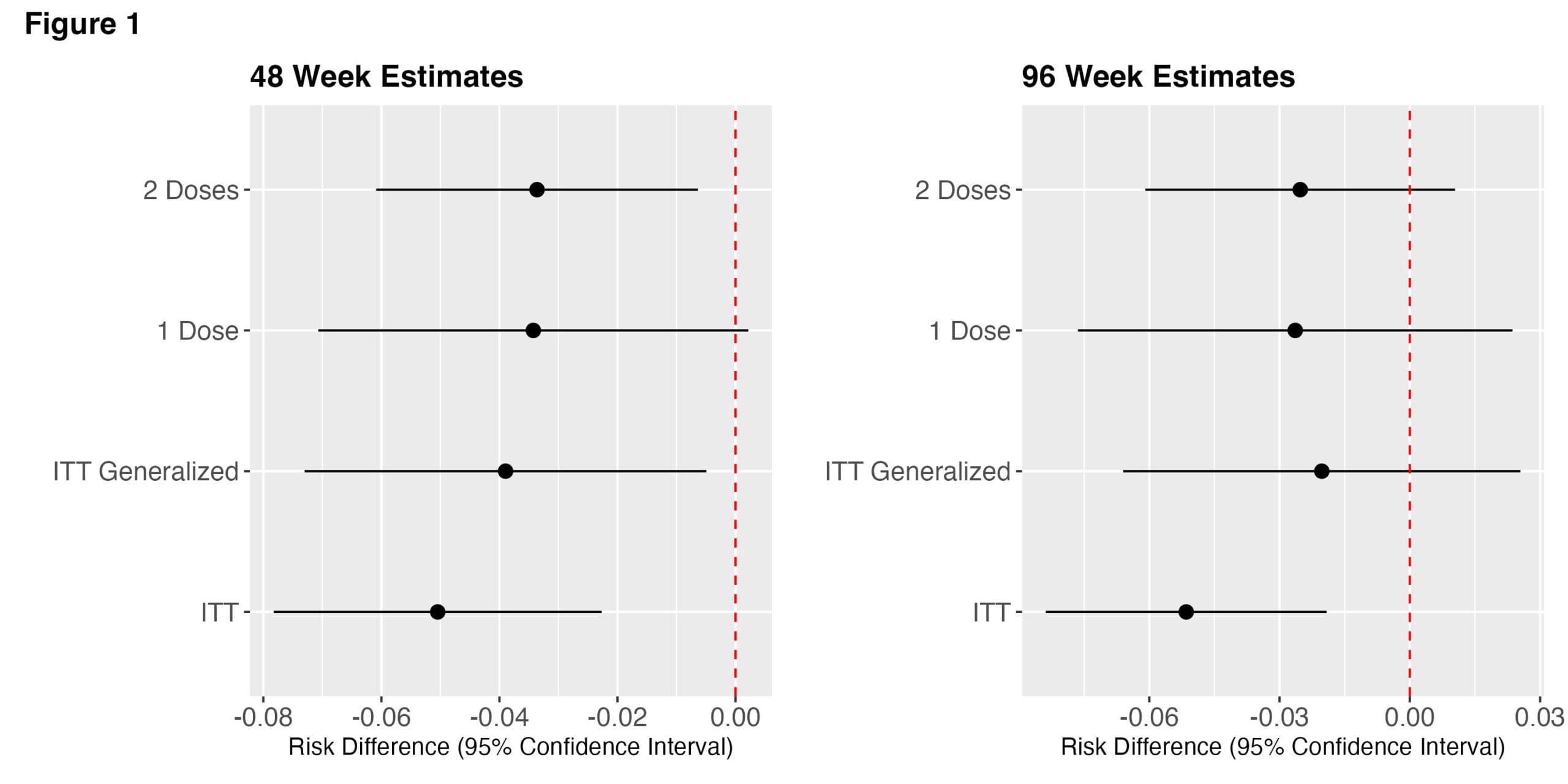
Results: 1857 participants from the A5202 were included. The mean age was 38 [IQR: 31-45], 83% were male, 58% white, and 34% were Black. Estimates are presented in Figure 1. At 48 weeks the ITT risk difference between TDF/FTC v. ABC/3TC was -0.050 (95% CI: -0.08, -0.02), but when generalized to the US population was -0.038 (95%CI: -0.07, -0.004). The generalized 1 dose and 2 dose protocol 48-week risk differences were -0.03 (95%CI: -0.07, 0.003) and -0.03 (95%CI: -0.06, -0.006), respectively. At 96 weeks the ITT risk difference between TDF/FTC v. ABC/3TC was -0.05 (95% CI: -0.08, -0.02). The generalized 1 dose and 2 dose protocol 96-week risk differences were -0.02 (95%CI: -0.07, 0.03) and -0.03 (95%CI: -0.06, 0.01), respectively.
Discussion: Per protocol analyses are infrequently done and very rarely consider multiple definitions of protocol. There were no meaningful differences when comparing risk differences between protocols in the study sample. However, when generalized to the target population with incident HIV, the A5202 risk difference estimates were closer to the null than the non-generalized results. These results may impact decisions about treatment efficacy in clinical care and expectations about subsequent treatment effects.