Multilevel predictors of telehealth and integrated primary care within behavioral health services, US, 2024
Abstract
Background
Integrated primary care (IPC) within behavioral health services helps address comorbidities that complicate treatment. Most behavioral health patients who need IPC don’t receive it. Telehealth has been shown to improve behavioral health access and outcomes, and telehealth combined with IPC is the next step in providing comprehensive behavioral healthcare. To date, no epidemiologic studies have assessed the prevalence of combined telehealth and IPC, or multilevel factors that promote its adoption.
Methods
We used the Mental Health and Addiction Treatment Tracking Repository to identify all known licensed substance use disorder and mental health outpatient treatment facilities in the US (2024; N=17,599 facilities). We used multilevel logistic regression to predict telehealth and IPC, using facility-level characteristics (owner type), census-tract-level characteristics (rurality, social vulnerability), county-level characteristics (broadband coverage), and state telehealth policies (modality-neutral, in-person requirements, state-line barriers, and nurse-independent practice). We included interactions between state policies, underserved communities, and treatment service type. State was defined as a random effect.
Results
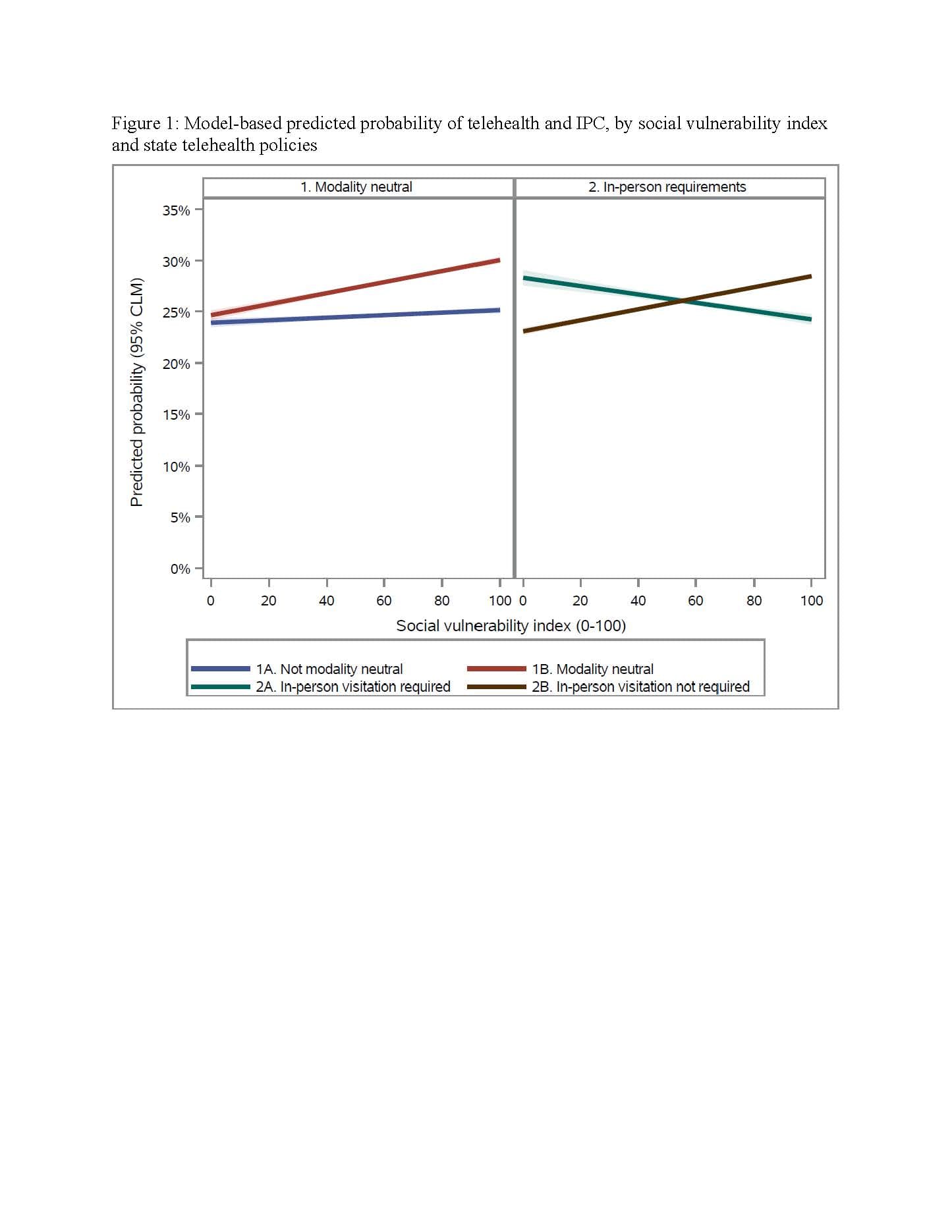
A quarter of treatment facilities offered telehealth and IPC. Facilities located in underserved communities were more likely to provide telehealth and IPC when their state had policies that allowed modality neutrality (interaction p=0.06) and allowed patients to start telehealth without an initial in-person visitation (interaction p<0.01; Figure 1).
Conclusion
State telehealth policies do not affect all communities within a state equally, as some policies are more advantageous to facilities serving more vulnerable populations. Policies that allow a range of telehealth modalities and do not require an initial in-person visit were more effective at improving access to telehealth and IPC among communities with higher vulnerability.