Ultrasound suspicion of fetal large for gestational age and maternal and neonatal outcomes
Abstract
Objective: To compare maternal and neonatal outcomes among large-for-gestational-age (LGA) neonates with and without prenatal ultrasound suspicion of LGA.
Study Design: We conducted a population-based cohort study of term LGA births in Ontario, Canada (2012–2021) using linked health administrative data. LGA births with documented prenatal ultrasound suspicion of LGA were treated as exposed and compared with LGA births without such documentation. Outcomes included labor interventions, maternal complications, and neonatal outcomes. Propensity scores with overlap weights were applied in modified Poisson regression models. To explore potential mediating factors and misclassification bias, sensitivity analyses included 1) removing gestational hypertension variables from the propensity score and 2) including those without a documented complication of suspected LGA but a late third trimester ultrasound to the exposed group.
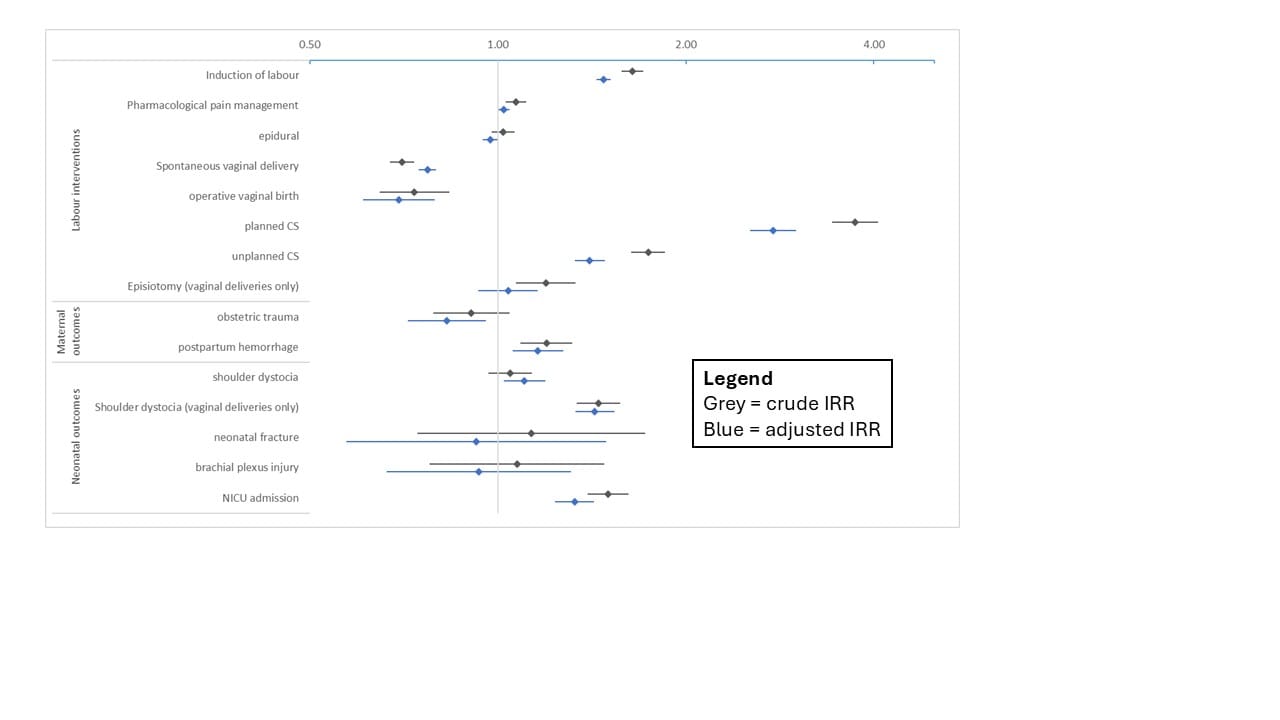
Results: Among 82,385 LGA births, 3,969 (4.8%) had prenatal ultrasound suspicion of LGA. After adjustment, suspected LGA had higher rates of labour induction (39.0% vs 64.0%; aIRR [adjusted incidence rate ratio] 1.48, 95% CI 1.44–1.52), planned cesarean delivery (4.3% vs 16.0%; 2.76, 2.54–3.00), unplanned cesarean delivery (15.9% vs 27.6%; 1.40, 1.33–1.48), postpartum hemorrhage (9.5% vs 11.4%; 1.16, 1.06–1.27), shoulder dystocia (15.4% vs 16.1%; 1.10, 1.02–1.19), and neonatal intensive care unit admission (12.1% vs 18.1%; 1.33, 1.23–1.43; Figure 1). Operative vaginal delivery and obstetric trauma rates were lower among deliveries with suspected LGA (8.2% vs 6.1%; 0.69, 0.61-0.79 and 5.7% vs 5.2%; 0.83, 0.72-0.96 respectively). Results from the two sensitivity analyses were similar to the main analysis.
Conclusion: Prenatal ultrasound suspicion of LGA is associated with increased interventions without improved maternal or neonatal outcomes other than a decrease in operative vaginal delivery and obstetric trauma.