Effect of Smoke-Free Laws on Cardiovascular Disease (CVD) Mortality in US counties, 2000–2018: An Application of the Generalized Synthetic Control Method
Abstract
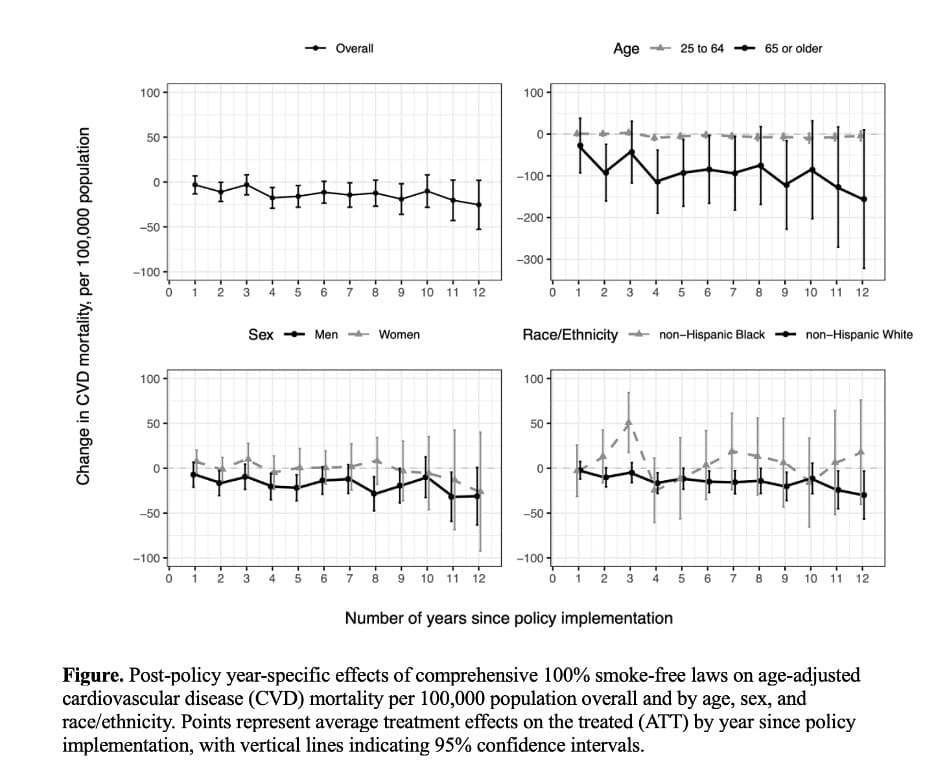
Comprehensive smoke-free laws reduce secondhand smoke exposure and may lower cardiovascular disease (CVD) risk, but long-term effects on cardiovascular disease (CVD) mortality and the distribution of benefits across subgroups remain uncertain. We estimate the long-term impact of comprehensive smoke-free laws on county-level CVD mortality and assess heterogeneity by age, sex, and race/ethnicity. We conducted a quasi-experimental study of U.S. counties from 2000–2018 using the generalized synthetic control method (GSCM) with staggered policy adoption. Treated counties (n=38) implemented comprehensive 100% smoke-free laws in workplaces, restaurants, and bars between 2007 and 2018, while control counties (n=103) never adopted such laws. The outcome was annual age-adjusted CVD mortality per 100,000 population (ICD-10 I00–I99), analyzed overall and stratified by age (25–64 years, ≥65 years), sex, and race/ethnicity. We estimated year-specific and 12-year averaged average treatment effects on the treated (ATTs) with bootstrapped 95% confidence intervals. Smoke-free laws were associated with sustained reductions in overall CVD mortality (12-year averaged ATT −12.0 per 100,000; 95% CI, −21.3 to −2.7). Larger reductions were observed among adults aged ≥65 years (ATT −84.4; 95% CI, −146.0 to −22.7), men (ATT −16.8; 95% CI, −26.5 to −7.0), and non-Hispanic White populations (ATT −12.6; 95% CI, −21.5 to −3.7). Effects among adults aged 25–64 years, women, and non-Hispanic Black populations were smaller and imprecise. Year-specific post-policy ATTs are shown in the Figure. Comprehensive smoke-free laws were associated with meaningful and durable declines in county-level CVD mortality, but benefits were uneven across demographic groups. Equity-focused implementation and enhanced protections are needed to address persistent disparities in second-hand smoke exposure and cardiovascular outcomes.