The Contribution of Cesarean Birth to Black-White Disparities in Severe Postpartum Hemorrhage
Abstract
Disparities in US maternal morbidity are well established and seen in a heightened risk for Black women for both cesarean section (CS) and its potential complications, like postpartum hemorrhage (PPH). It remains unclear whether disparities in PPH are driven primarily by higher CS prevalence or higher risk of PPH following CS.
We used 2016–2022 National Inpatient Sample data to examine the contributions of CS to the Black–White disparity in severe PPH (SPPH: PPH with shock, hysterectomy, or disseminated intravascular coagulopathy). The sample comprised 2,672,991 singleton, term, cephalic deliveries to non-Hispanic Black and White women without indications for CS for hemorrhage risk. Race-stratified adjusted linear probability models estimated risk differences in SPPH across maternal and hospital characteristics. Oaxaca-Blinder decomposition analyses quantified the proportion of the Black–White disparity in SPPH accounted for by measured factors. Analyses were further stratified by year (2016-19 and 2020-22) and repeated among a subgroup of 2,212,257 deliveries with no prior CS.
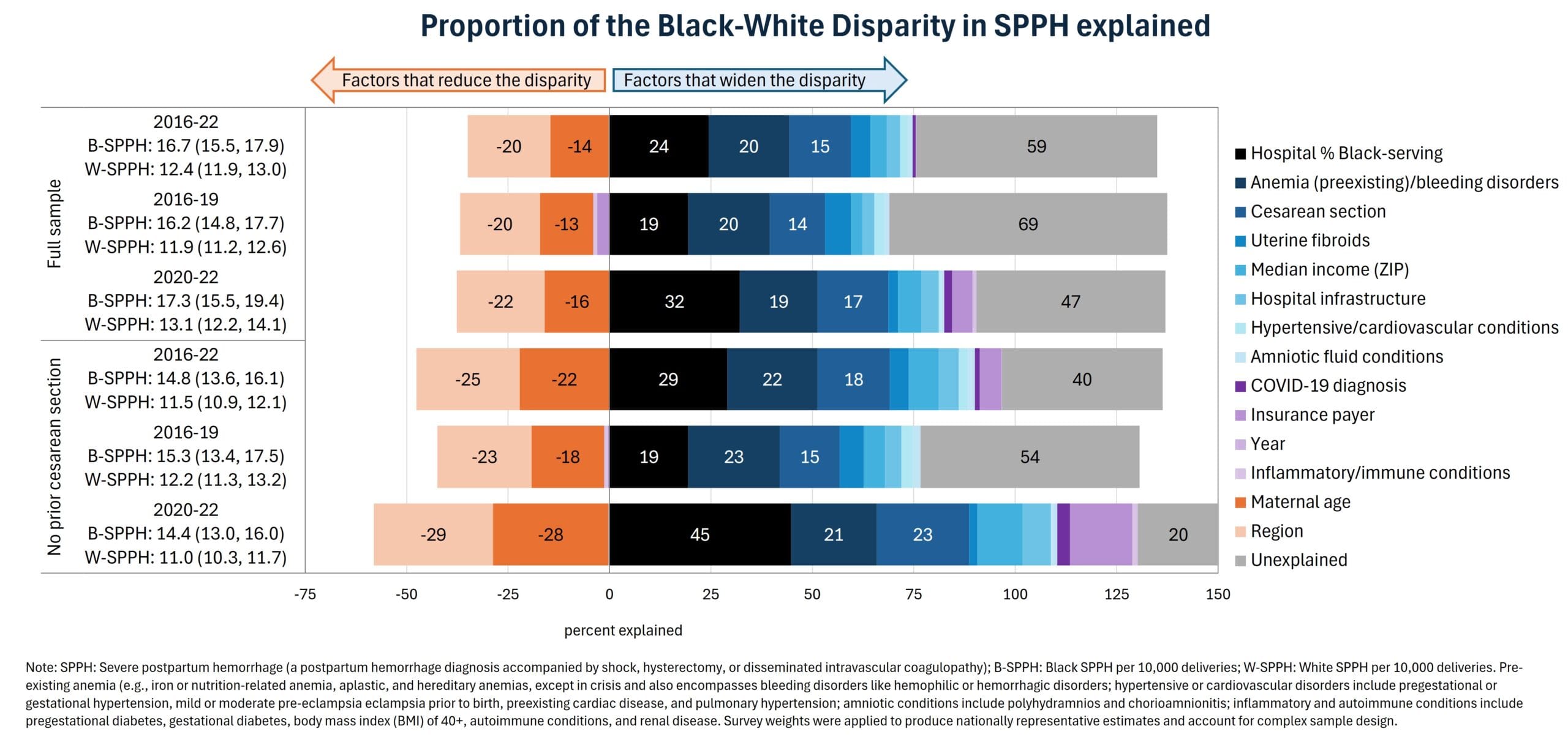
SPPH befell 16.6 (95% CI: 15.5-17.8) and 12.4 (95% CI: 11.8-13.0) per 10,000 deliveries to Black and White women, respectively. CS was associated with higher risk of SPPH for both races. Overall, CS, pre-existing anemia, and higher hospital percent Black-serving patients were the largest contributors to the Black–White SPPH disparity (15%, 20%, and 24%, respectively). Age and regional distribution attenuated the disparity; 59% was unexplained by measured factors (Figure). In 2020-22, COVID diagnoses contributed little (2%), but the contribution of greater Black-serving hospitals grew to 32%, leaving less unexplained. Subgroup analyses (no prior CS) found similar patterns but a smaller Black-White disparity in SPPH (14.8 vs. 11.5 per 10,000).
With stark racial disparities in severe maternal morbidity, interventions to improve access to high-quality, equitable maternity care are urgently needed.