Disparities in spatial access to Hepatitis C treatment providers, Los Angeles County
Abstract
Background: Access to hepatitis C virus (HCV) treatment is essential for patients to get a cure, prevent transmission, and advance elimination efforts in the United States, yet evidence on spatial access to HCV treatment remains limited.
Objective: To assess variation in spatial access to HCV treatment providers across zip code tabulation areas in Los Angeles County and socioeconomic factors correlated with low access.
Methods: In this cross-sectional study, we combined provider location data, the reported rate of HCV infection, and American Community Survey data to assess spatial access to treatment providers. Potential treatment providers were identified through the National Plan and Provider Enumeration System, which included specialists (hepatologists, gastroenterologists, and infectious disease specialists) and non-specialists, such as primary care physicians and advanced practice providers, 2023. For each zip code, spatial access ratios to providers were calculated using the Enhanced 2-step Floating Catchment Area method. Hotspot analysis (Getis-Ord Gi*) was employed to identify and visualize clusters of low and high spatial access. Zip codes were classified into three access categories (low, moderate, and high-access areas) based on the mean and standard deviation of the spatial access ratios. Multinomial regression assessed socioeconomic factors associated with low spatial access, defined as a spatial access ratio more than one standard deviation below the county mean.
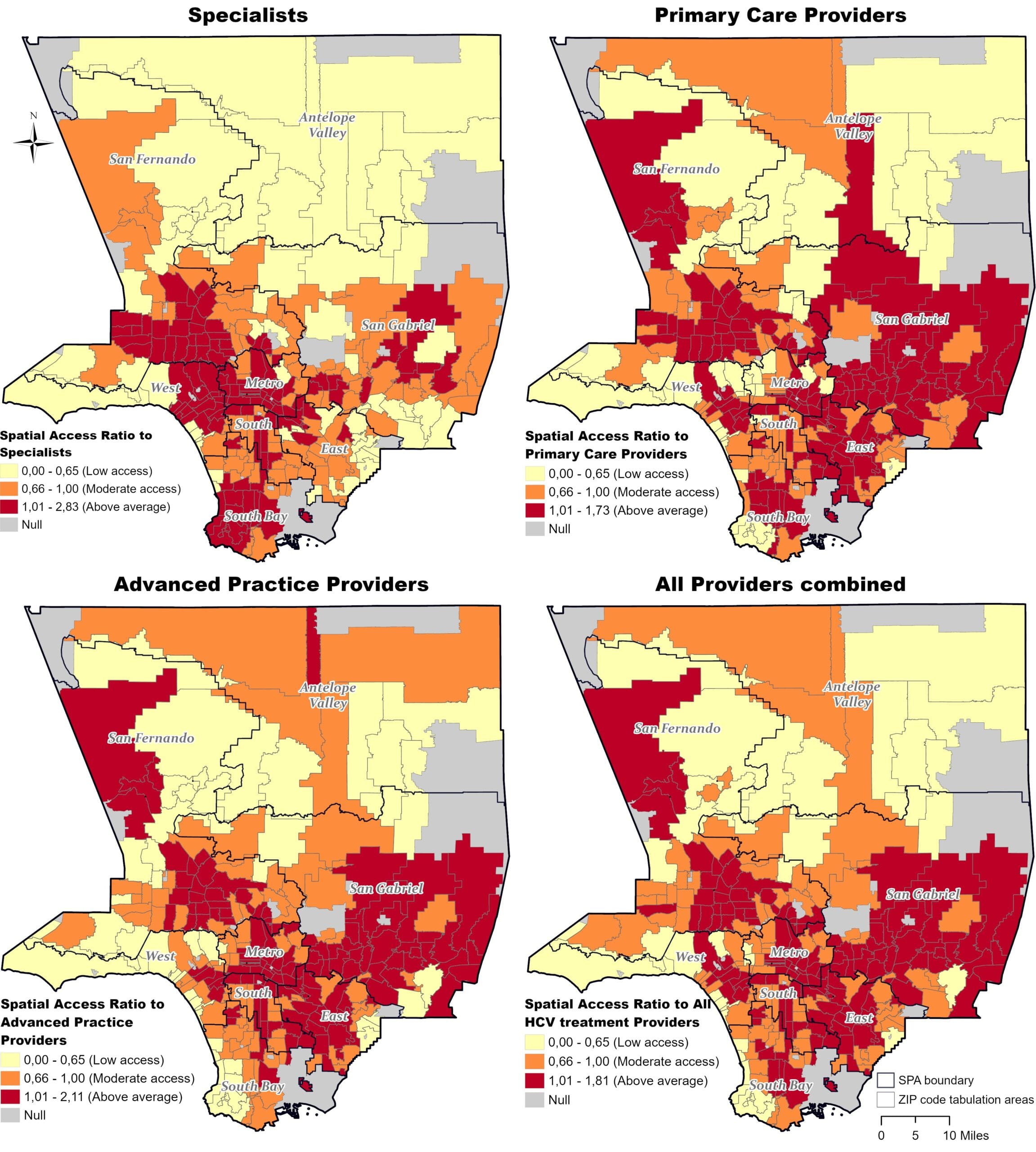
Results: A total of 6,826 providers were included in the analysis, comprising 614 specialists, 2,531 primary care physicians, and 3,682 advanced practice providers. Among the 255 zip codes examined, 13% were classified as low-access areas, 34% as moderate-access, and 53% as high-access, considering access to all providers combined. Considering spatial access to provider types separately, access to non-specialists was generally higher than access to specialists. Notably, for access to specialists, 20% of the zip codes were classified as low-access; for advanced practice providers and primary care providers, 17% and 15% of zip codes were classified as low-access, respectively. High-access areas for specialists were primarily located on the west side of the county, whereas high-access areas for non-specialists were distributed more broadly throughout the county. Factors correlated with increased likelihood of low-access to all providers were higher poverty levels, uninsured residents, and a higher share of Hispanic residents.
Conclusion: Spatial access to HCV treatment providers in Los Angeles County reveals significant disparities; while access to non-specialists is relatively geographically equitable, specialists are concentrated in specific areas. This highlights the potential of non-specialists to enhance treatment coverage in underserved regions. The Enhanced 2-step Floating Catchment Area offers a valuable approach for assessing geographic disparities in access to HCV treatment providers.