Estimating dementia-related outcomes among patients following hospitalization with septic shock
Abstract
Septic shock (SS) is a leading global cause of morbidity and mortality, yet its long-term cognitive and functional consequences remain underexplored. Emerging evidence suggests an association between SS and an increased risk of dementia, but causal interpretation is limited by the lack of appropriate comparator groups, as SS is not a well-defined exposure and is closely intertwined with hospitalization, comorbidities, and shared vascular risk factors.
Using longitudinal data from NIH’s All of Us Research Program, we emulated a series of target trials to compare the hazard of dementia following SS-related hospitalization versus other acute illness-related hospitalizations. Comparator groups included those hospitalized for myocardial infarction (AMI), renal failure (ARF), and pulmonary edema (APE), representing alternative acute illness trajectories sharing features of severe hospitalization but differing in underlying biological mechanisms. Dementia-free adults ≥18 years (N = 52,447) were followed from time of hospitalization, with dementia defined using ICD-9/10 codes. Cox models estimated cause-specific hazard ratios, adjusting for demographic, comorbidity, and SES variables.
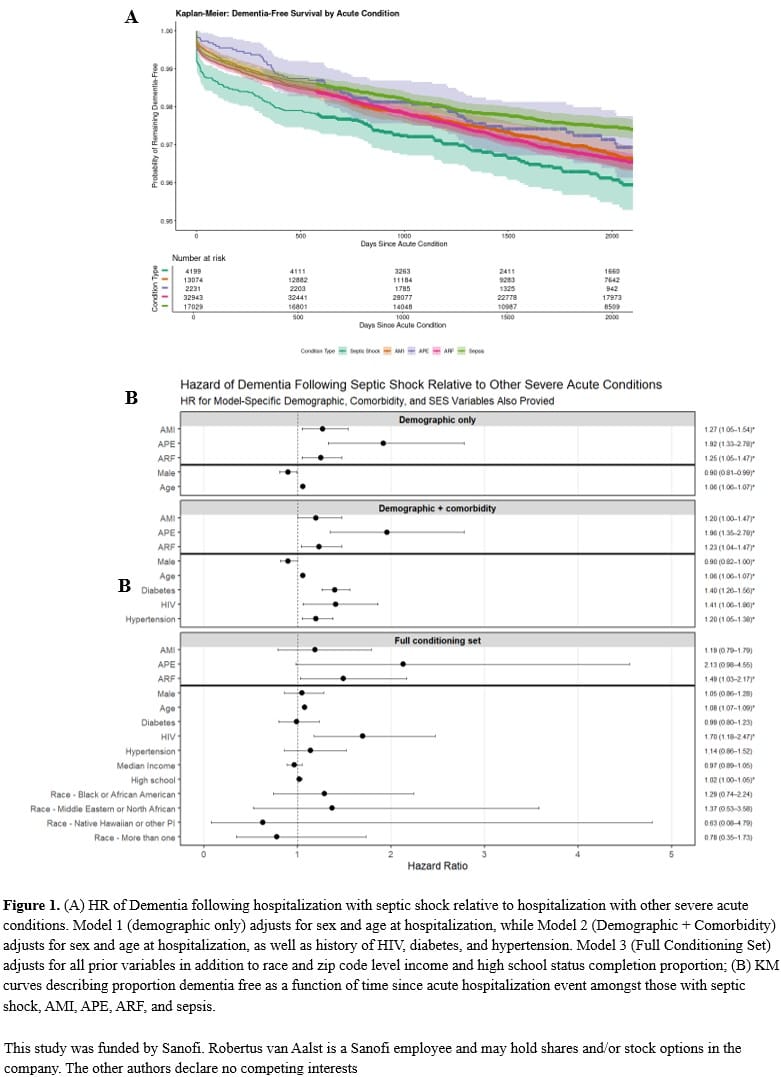
SS hospitalization was associated with a higher hazard of dementia compared to non-infectious acute hospitalizations. Sepsis was significantly associated with increased dementia hazard compared to ARF (HR: 1.49, 95% CI: 1.03-2.17). Point estimates suggested notable differences versus APE (HR: 2.13, CI: 0.98-4.55) and AMI (HR: 1.19, CI: 0.97-1.79), though these were not statistically significant. Results were robust to alternative covariate adjustment.
Using an ICD-9/10-based definition of SS and multiple comparator groups, this study clarifies how the hazard of dementia differs after SS compared with other acute hospitalizations. These findings suggest that SS-specific mechanisms, beyond the general effects of critical illness and hospitalization, may contribute to long-term cognitive decline.