HIV / STI
HIV Status and Cardiometabolic Comorbidities among Reproductive Aged Women in the STAR Cohort Danielle J. Carson* Angela Bengtson Danielle J. Carson Lauren F. Collins Christina C. Mehta Seble G. Kassaye Aadia Rana Daniel Westreich Elizabeth F. Topper Maria L. Alcaide Anandi N. Sheth
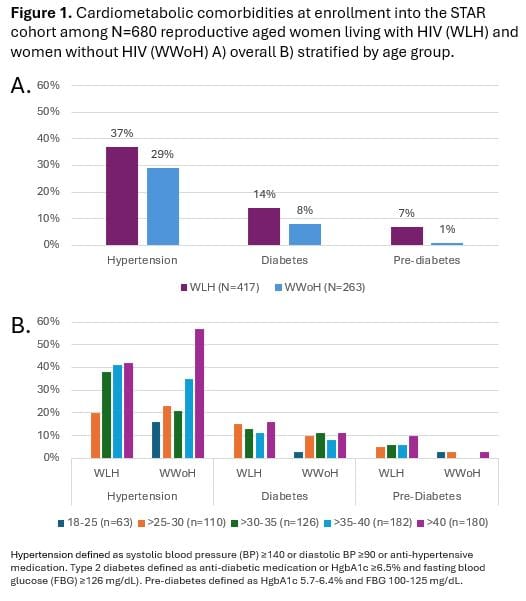
Women living with HIV (WLH) are at greater risk of cardiometabolic comorbidities than women living without HIV (WWoH) and may experience these conditions at younger ages. However, little is known about the burden of cardiometabolic comorbidities in WLH of reproductive age. Using data from the Study of Treatment and Reproductive Outcomes in Women (STAR) cohort, including WLW and WWoH across 6 sites in the Southeast United States, we assessed the prevalence of cardiometabolic comorbidities at enrollment, evaluated associations between HIV status using multivariable log binomial models, and explored effect modification by age. Cardiometabolic comorbidities were evaluated at cohort enrollment and included: 1) hypertension (systolic blood pressure (BP) ≥140 or diastolic BP ≥90 (international standard) or anti-hypertensive medication); 2) type 2 diabetes (anti-diabetic medication or HgbA1c ≥6.5% and fasting blood glucose (FBG) ≥126 mg/dL); 3) pre-diabetes (HgbA1c 5.7-6.4% and FBG 100-125 mg/dL). Among 680 women (417 WLH, 263 WWoH) at enrollment, the median age was 37 (IQR 30,41), median BMI was 32 kg/m2 (IQR 26, 42), and 75% identified as non-Hispanic Black race. Compared to WWoH in unadjusted analyses, WLH had a higher prevalence of hypertension (37% vs 29%), diabetes (14% vs 8%) and pre-diabetes (7% vs 1%) (Figure 1A) and had a higher prevalence of these comorbidities at younger ages (Figure 1B). After adjustment for age, obesity status, education, and ever smoking, HIV was not associated with prevalent hypertension (PR 0.85 95% CI 0.64, 1.13) or diabetes (PR 1.33 95% CI 0.70, 2.54) but was associated with prevalent pre-diabetes (PR 4.11 95% CI 1.20, 14.03), although precision was limited. In this diverse cohort of reproductive-aged WLH and WWoH, the burden of cardiometabolic comorbidities was high. Longitudinal follow-up is needed to determine how HIV status affects the incidence and age at onset of cardiometabolic comorbidities in reproductive-aged women.