Health Disparities
Geographic variation in intersectional racial and gender disparities in access to the kidney transplant waitlist in the US Annika Gompers* Annika Gompers Kaitlyn Stanhope Jessica Harding
Background: Kidney transplantation is lifesaving treatment for people living with kidney failure, however access is not equitable by race, gender, and their intersection. The objective of this study was to examine US state-level variation in intersectional racial and gender disparities in access to the kidney transplant waitlist.
Methods: We used the US Renal Data System to conduct a retrospective cohort study of all Black or white adults initiating kidney replacement therapy (KRT; dialysis or transplantation) in the US from 2015 through 2019, with follow-up through 2021. We estimated predicted probabilities of waitlisting in each race-gender group (Black women, Black men, white women, white men) and categorized their rank order. For US-wide estimates, we used generalized estimating equations to fit Cox proportional hazard models accounting for clustering by state. For state-specific estimates, we fit Cox proportional hazard models with an interaction term between race-gender group and state. We adjusted for individual clinical and social factors, dialysis facility characteristics, and neighborhood characteristics.
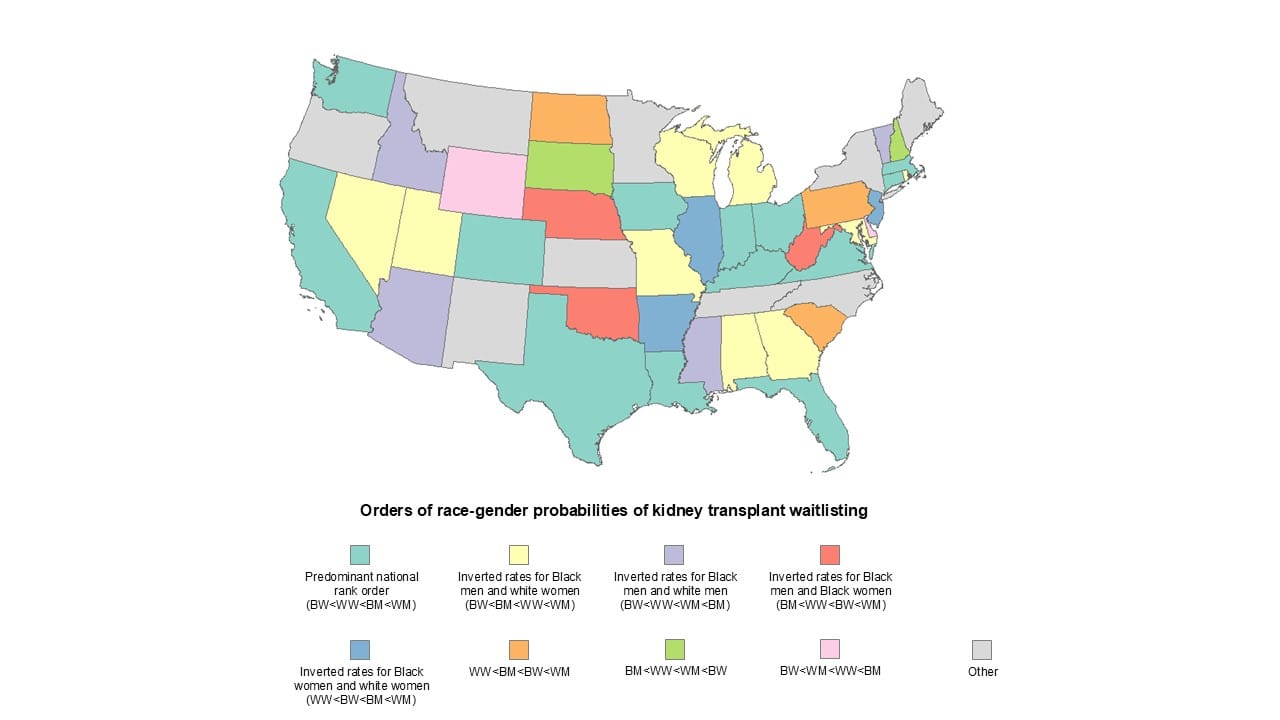
Results: Among 488,400 patients initiating KRT, the adjusted probability of waitlisting within 3 years was lowest among Black women (0.115 [95% CI 0.111-0.120]), followed by white women (0.123 [0.117-0.129]), Black men (0.128 [0.123-0.134]), then white men (0.141 [0.136-0.147]). There was heterogeneity in the rank order of waitlisting probabilities found in each US state (Figure 1). In 31 states the lowest probability was among Black women, in 11 states it was lowest among white women, and in 8 states it was lowest among Black men; white men did not have the lowest probability of waitlisting in any state.
Conclusion: Substantial geographic variation exists in intersectional racial and gender disparities kidney transplant access in the US, indicating that potentially intervenable state-level conditions may contribute to these disparities.